Opioid Use Disorder:
Definition:
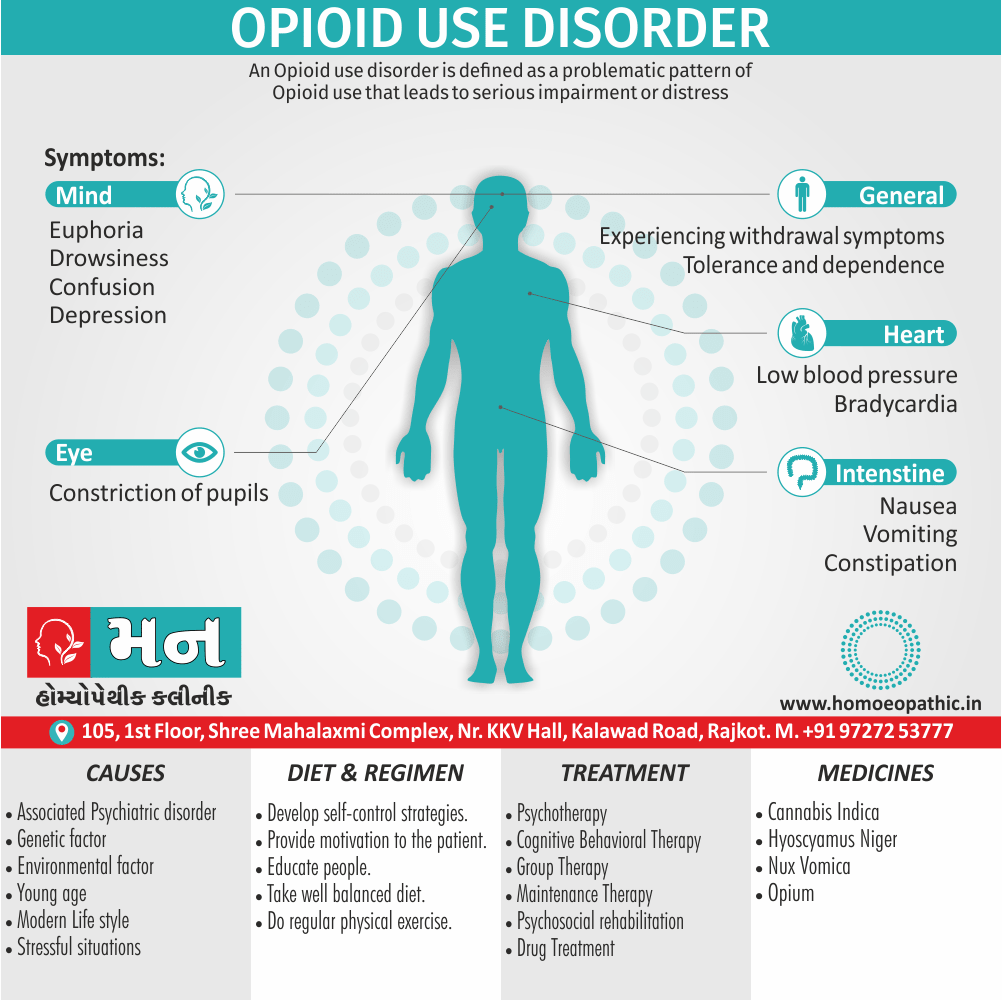
Opioids are substances that mimic the effects of endogenous opioids (endorphins also enkephalins) by acting as agonists at the opioid receptors. [1]
Overview
In the last few decades, opioid use disorder has increased markedly all over the world. [2]
The first record of opioid use by humans was in Mesopotamia in around 3400 BC, when people extracted the natural opioids from poppies and smoked them.
Originally it was marketed as a less addictive form of morphine, but unfortunately this turned out to be completely wrong. Diamorphine is the mostly widely used opioid, as it produces the most powerful euphoria. [1]
Dried exudate obtained from unripe seed capsules of Papaver somniferum has used also abused for centuries. Additionally; The natural alkaloids of opium and their synthetic preparations are highly dependence producing. [2]
Worldwide spread
The UN estimates that 15–20 million people worldwide are dependent upon diamorphine at any one time. As well as the desired euphoric effect of opioids, they also have a wide range of other effects upon the body, with the most commonly experienced being analgesia, constipation, anorexia, and loss of libido.
All in all; The high risk of respiratory depression makes the uncontrolled use of opioids very dangerous. [1]
A. Natural Alkaloids of Opium:
- Morphine
- Codeine
- Thebaine
- Noscapine
- Papaverine
B. Synthetic Compounds:
- Heroin
- Nalorphine
- Hydromorphone
- Methadone
- Dextropropoxyphene
- Meperidine (in other words; Pethidine)
- Cyclazocine
- Levallorphan
- Diphenoxylate
The most important dependence producing derivatives are morphine and heroin. They both like majority of dependence producing opioids bind to μ (mu) opioid receptors. The other opioid receptors are k (kappa, e.g. for pentazocine), δ (delta, e.g. for a type of enkephalin), σ (sigma, e.g. for phencyclidine), ε (epsilon) and λ (lambda). [2]
Psychological and neurological:
- Tolerance also dependence
- Anxiolysis
- Either Confusion or delirium
- Euphoria
- Drowsiness
- Analgesia
Cardiovascular:
Bradycardia
Hypotension
Respiratory:
Respiratory depression
Hypoventilation
Gastrointestinal:
Nausea also vomiting
Constipation
Dyspepsia
Miscellaneous:
Dry mouth
Pupil constriction
Urinary retention
Muscle spasticity
Itching. [1]
Opioids can be taken by mouth, intravenously, either by inhaling, or by smoking.
-
Mouth:
When diamorphine is taken orally it undergoes extensive first-pass metabolism, converting it to morphine and reducing the euphoric effects.
-
Intravenous (IV):
Intravenous (IV) use avoids this metabolism, and diamorphine crosses the blood–brain barrier quickly and produces a rapid powerful euphoria. IV use of heroin carries all of the risks discussed earlier in the chapter.
The antecubital fossa is usually the site first used for injecting, but eventually the veins become damaged and the user moves elsewhere.
- When venous access becomes extremely difficult, users may inject either subcutaneously (skin popping) or intramuscularly. [1]
- Apart from the parenteral mode of administration, heroin can also be smoked or ‘chased’ (chasing the dragon), often in an impure form (called ‘ smack’ or ‘ brown sugar’ in India). [2]
The form of heroin most commonly used in the UK will only dissolve if mixed with an acid and heated. The use of citric acid powder and lemon juice is typical, with heating occurring on a spoon over a heat source.
The use of acids is particularly troublesome because it causes immense damage to the veins. [1]
Heroin or di-acetyl-morphine is about two times more potent than morphine in inject-able form.
Duration
Heroin is more addicting than morphine and can cause dependence even after a short period of exposure. Tolerance to heroin occurs rapidly and can be increased to up to more than 100 times the first dose needed to produce an effect. [2]
Intoxication is characterised by apathy, bradycardia, hypotension, respiratory depression, subnormal core body temperature, also pin-point pupils.
Later, delayed reflexes, thready pulse and coma may occur in case of a large overdose. In severe intoxication, mydriasis may occur due to hypoxia. [2]
Before treatment, a correct diagnosis must be made on the basis of history, examination (pin-point pupils during intoxication or withdrawal symptoms) and/or laboratory tests.
These tests are:
- Naloxone challenge test (to precipitate withdrawal symptoms).
- Urinary opioids testing:
With radioimmunoassay (RIA), free radical assay technique (FRAT), thin layer chromatography (TLC), gas-liquid chromatography (GLC), high pressure liquid chromatography (HPLC) or enzyme-multiplied immunoassay technique (EMIT). [2]
The onset of withdrawal symptoms occurs typically within 12-24 hours, peaks within 24-72 hours, and symptoms usually subside within 7-10 days of the last dose of opioid.
The characteristic symptoms include i.e.:
- Lacrimation
- Intense craving for the drug
- Rhinorrhoea
- Pupillary dilation
- Sweating
- Diarrhoea
- Yawning
- Tachycardia
- Mild hypertension
- Insomnia
- Raised body temperature
- Muscle cramps
- Generalised bodyache
- Severe anxiety
- Piloerection
- Nausea
- Vomiting
- Anorexia
In detail; There are marked individual differences in presentation of withdrawal symptoms. Additionally, Heroin withdrawal syndrome is far more severe than the withdrawal syndrome seen with morphine. [2]
Biological:
Infections e.g.:
- Abscesses and cellulitis
- Sepsis
- HIV
- Hepatitis B or C
- Bacterial endocarditis
Cardiorespiratory e.g.:
- Deep vein thrombosis or embolism
- Aspiration
- Respiratory depression
- Cardiac arrhythmias
Complications of pregnancy
Death from overdose
Psychological:
- Depression
- Anxiety disorders
- Deliberate self-harm
- Suicide
Social:
- Unemployment
- Loss of accommodation
- Breakdown of relationships
- Loss of friends
- Criminal record [1]
The treatment can be divided into three main types:
1. Firstly; Treatment of overdose.
2. Secondly; Detoxification.
3. Thirdly; Maintenance therapy.
1. Treatment of Opioid Overdose:
The key clinical findings in a patient who has taken an overdose of opioids are:
- Respiratory depression (rate less than eight breaths per minute), possibly leading to respiratory arrest
- Unreactive pinpoint pupils
- Bradycardia
- Hypotension
- Snoring or other upper airway sounds
- Reduced level of consciousness.
Patients should be approached using the principles of airway, breathing, also circulation and treated with oxygen, respiratory support, fluids, and inotropes if necessary. [1]
An overdose of opioid can treated with narcotic antagonists (such as naloxone, naltrexone). Additionally; Usually an intravenous injection of 2 mg naloxone, followed by a repeat injection in 5-10 minutes, can cause reversal of overdose.
But as naloxone has a short half-life repeated doses may be needed every 1-2 hours. Lastly; This should combined with general care and supportive treatment. [2]
2. Detoxification (Planned withdrawal of opioids):
This is a mode of treatment in which the dependent person is ‘taken off’ opioids. In detail; This is usually done abruptly, followed by management of emergent withdrawal symptoms.
It is highly recommend that detoxification is conduct in a safe manner under expert guidance of a specialist.
The withdrawal symptoms can managed by one of the following methods i.e.:
Use of substitution drugs i.e.:
Such as methadone to ameliorate the withdrawal symptoms. The aim is to gradually taper off the patient from methadone (which is less addicting, has a longer half-life, decreases possible criminal behaviour, and has a much milder withdrawal syndrome).
However, relapses are common and its opponents argue that one type of dependence is often replaced by another (methadone).
Clonidine i.e.:
Basically; It is an α2 agonist that acts by inhibiting norepinephrine release at presynaptic α2 receptors. The usual dose is 0.3-1.2 mg/day, also drug is tapered off in 10-14 days.
It can be started after stoppage of either the opioid itself or the substitution drug (for example; methadone). The important side effects of clonidine are excessive sedation and postural hypotension.
Lastly; Clonidine treatment is usually started in an inpatient psychiatric or specialist alcohol and drug treatment center setting.
Naltrexone with Clonidine i.e.:
Naltrexone is an orally available narcotic antagonist which, when give to an opioid dependent individual, causes withdrawal symptoms. These symptoms are manage with the addition of clonidine for 10-14 days after which clonidine is withdraw and the patient is continue on naltrexone alone.
Now if the person takes an opioid, there are no pleasurable experiences, as the opioid receptors are block by naltrexone.
Therefore, this method is a combination of detoxification and maintenance treatment. The usual dose of naltrexone is 100 mg orally, administered on alternate days.
Other Drugs i.e.:
The other detoxification agents include LAAM (levo-alpha-acetyl-methadol), propoxyphene, diphenoxylate, buprenorphine (long acting synthetic partial μ-agonist which can be administered sublingually), and lofexidine (α2 agonist, similar to clonidine).
In particular, Buprenorphine has recently used widely for detoxification as well as for maintenance treatment in many parts of the World. Care must be exercised as there is potential for misuse with buprenorphine. [2]
When heroin is withdrawn, psychological support is particularly important to avoid immediate relapse. Withdrawal usually undertaken by substituting methadone (a longer-acting drug) for heroin.[1]
3. Maintenance Therapy:
After the detoxification phase is over, the patient is maintain on one of the following regimens:
Methadone maintenance (Agonist substitution therapy) i.e.:
This a very popular method use widely in the Western World. 20-50 mg/day of methadone is give to the patients to ‘shift’ them from ‘hard’ drugs, thus decreasing IV use and criminal behaviour.
Its use in India has not recommended by an expert committee for de-addiction services. Other drugs such as LAAM and buprenorphine can used for maintenance treatment.
Opioid antagonists i.e.:
Opioid antagonists have in use for a long time but they were either partial antagonists (such as n alorphine) or had to administer parenterally (such as naloxone).
Furthermore; The usual maintenance dose is 100 mg on Mondays and Wednesdays, and 150 mg on Fridays.
Naltrexone combine with clonidine, as describe above, is a very effective method for detoxification as well as for maintenance treatment.
Other methods i.e.:
These include individual psychotherapy, behaviour therapy, interpersonal therapy, cognitive behaviour therapy (CBT), motivational enhancement therapy, self-control strategies, psychotropic drugs for associated psychopathology, family therapy, and group therapy (e.g. in therapeutic communities such as Synanon, self-help groups such as Narcotic Anonymous or NA).
These methods have to tailored for use in an individual patient.
Psychosocial rehabilitation i.e.:
This is a very important step in the post-detoxification phase, in the absence of which relapse rates can very high. Rehabilitation should at both occupational and social levels. [2]
Frequently Asked Questions
What is Opioid Use Disorder?
Opioids are substances that mimic the effects of endogenous opioids (endorphins and enkephalins) by acting as agonists at the opioid receptors.
Name of the derivatives of Opioid?
- Morphine
- Codeine
- Thebaine
- Noscapine
- Papaverine
- Heroin
- Nalorphine
- Hydromorphone
- Methadone
What is Acute Intoxication of Opioid Use Disorder?
- Apathy
- Bradycardia
- Hypotension
- Respiratory depression
- Subnormal core body temperature
- Pin-point pupils
What is Withdrawal Syndrome of Opioid Use Disorder?
- Psychiatry, Fourth Edition- Oxford Medical Publications – SRG- by Geddes, Jonathan Price, Rebecca McKnight / Ch 29.
- A Short Textbook of Psychiatry by Niraj Ahuja / Ch 4
Definition: Opioids are substances that mimic the effects of endogenous opioids (endorphins also enkephalins) by acting as agonists at the opioid receptors. [1]
Overview
Opioid Derivatives
Physiological effects
Route of Administration
Acute Intoxication
Epidemiology
Causes
Risk Factors
Pathogenesis
Pathophysiology
Types
Clinical Features
Sign & Symptoms
Clinical Examination
Diagnosis
Differential Diagnosis
Withdrawal Syndrome
Complications
Investigations
Treatment
Prevention
Homeopathic Treatment
Diet & Regimen
Do’s and Dont’s
Terminology
References
FAQ
Also Search As
Overview
Overview
In the last few decades, opioid use disorder has increased markedly all over the world. [2]
The first record of opioid use by humans was in Mesopotamia in around 3400 BC, when people extracted the natural opioids from poppies and smoked them.
Originally it was marketed as a less addictive form of morphine, but unfortunately this turned out to be completely wrong. Diamorphine is the mostly widely used opioid, as it produces the most powerful euphoria. [1]
Dried exudate obtained from unripe seed capsules of Papaver somniferum has used also abused for centuries. Additionally; The natural alkaloids of opium and their synthetic preparations are highly dependence producing. [2]
Worldwide spread
The UN estimates that 15–20 million people worldwide are dependent upon diamorphine at any one time. As well as the desired euphoric effect of opioids, they also have a wide range of other effects upon the body, with the most commonly experienced being analgesia, constipation, anorexia, and loss of libido.
All in all; The high risk of respiratory depression makes the uncontrolled use of opioids very dangerous. [1]
Opioid Derivatives
A. Natural Alkaloids of Opium:
- Morphine
- Codeine
- Thebaine
- Noscapine
- Papaverine
B. Synthetic Compounds:
- Heroin
- Nalorphine
- Hydromorphone
- Methadone
- Dextropropoxyphene
- Meperidine (in other words; Pethidine)
- Cyclazocine
- Levallorphan
- Diphenoxylate
The most important dependence producing derivatives are morphine and heroin. They both like majority of dependence producing opioids bind to μ (mu) opioid receptors. The other opioid receptors are k (kappa, e.g. for pentazocine), δ (delta, e.g. for a type of enkephalin), σ (sigma, e.g. for phencyclidine), ε (epsilon) and λ (lambda). [2]
Physiological effects
Psychological and neurological:
- Tolerance also dependence
- Anxiolysis
- Either Confusion or delirium
- Euphoria
- Drowsiness
- Analgesia
Cardiovascular:
Bradycardia
Hypotension
Respiratory:
Respiratory depression
Hypoventilation
Gastrointestinal:
Nausea also vomiting
Constipation
Dyspepsia
Miscellaneous:
Dry mouth
Pupil constriction
Urinary retention
Muscle spasticity
Itching. [1]
Route of Administration
Opioids can be taken by mouth, intravenously, either by inhaling, or by smoking.
Mouth:
When diamorphine is taken orally it undergoes extensive first-pass metabolism, converting it to morphine and reducing the euphoric effects.
Intravenous (IV):
Intravenous (IV) use avoids this metabolism, and diamorphine crosses the blood–brain barrier quickly and produces a rapid powerful euphoria. IV use of heroin carries all of the risks discussed earlier in the chapter.
The antecubital fossa is usually the site first used for injecting, but eventually the veins become damaged and the user moves elsewhere.
- When venous access becomes extremely difficult, users may inject either subcutaneously (skin popping) or intramuscularly. [1]
- Apart from the parenteral mode of administration, heroin can also be smoked or ‘chased’ (chasing the dragon), often in an impure form (called ‘ smack’ or ‘ brown sugar’ in India). [2]
The form of heroin most commonly used in the UK will only dissolve if mixed with an acid and heated. The use of citric acid powder and lemon juice is typical, with heating occurring on a spoon over a heat source.
The use of acids is particularly troublesome because it causes immense damage to the veins. [1]
Heroin or di-acetyl-morphine is about two times more potent than morphine in inject-able form.
Duration
Heroin is more addicting than morphine and can cause dependence even after a short period of exposure. Tolerance to heroin occurs rapidly and can be increased to up to more than 100 times the first dose needed to produce an effect. [2]
Acute Intoxication
Intoxication is characterised by apathy, bradycardia, hypotension, respiratory depression, subnormal core body temperature, also pin-point pupils.
Later, delayed reflexes, thready pulse and coma may occur in case of a large overdose. In severe intoxication, mydriasis may occur due to hypoxia. [2]
Epidemiology
Indian epidemiology then other
Causes
This refers to the initiating factors that trigger a disease process.
- Examples of causes include:
- Pathogens: Viruses, bacteria, fungi, parasites (infectious diseases)
- Genetic mutations: Inherited or spontaneous changes in genes (genetic diseases)
- Environmental factors: Toxins, radiation, nutritional deficiencies
- Lifestyle choices: Smoking, unhealthy diet, lack of exercise (contributing factors)
Risk Factors
Risk factors are things that make you more likely to develop a disease in the first place.
Pathogenesis
Pathogenesis refers to the development of a disease. It’s the story of how a disease gets started and progresses.
This is the entire journey of a disease, encompassing the cause but going beyond it.
Pathophysiology
Pathophysiology, on the other hand, focuses on the functional changes that occur in the body due to the disease. It explains how the disease disrupts normal physiological processes and how this disruption leads to the signs and symptoms we see.
Imagine a car accident. Pathogenesis would be like understanding how the accident happened – what caused it, the sequence of events (e.g., one car ran a red light, then hit another car). Pathophysiology would be like understanding the damage caused by the accident – the bent fenders, deployed airbags, and any injuries to the passengers.
In simpler terms, pathogenesis is about the "why" of a disease, while pathophysiology is about the "how" of the disease’s effects.
Types
AAA
Clinical Features
Tab Content
Sign & Symptoms
Tab Content
Clinical Examination
Tab Content
Diagnosis
Before treatment, a correct diagnosis must be made on the basis of history, examination (pin-point pupils during intoxication or withdrawal symptoms) and/or laboratory tests.
These tests are:
- Naloxone challenge test (to precipitate withdrawal symptoms).
- Urinary opioids testing:
With radioimmunoassay (RIA), free radical assay technique (FRAT), thin layer chromatography (TLC), gas-liquid chromatography (GLC), high pressure liquid chromatography (HPLC) or enzyme-multiplied immunoassay technique (EMIT). [2]
Differential Diagnosis
Withdrawal Syndrome
The onset of withdrawal symptoms occurs typically within 12-24 hours, peaks within 24-72 hours, and symptoms usually subside within 7-10 days of the last dose of opioid.
The characteristic symptoms include i.e.:
- Lacrimation
- Intense craving for the drug
- Rhinorrhoea
- Pupillary dilation
- Sweating
- Diarrhoea
- Yawning
- Tachycardia
- Mild hypertension
- Insomnia
- Raised body temperature
- Muscle cramps
- Generalised bodyache
- Severe anxiety
- Piloerection
- Nausea
- Vomiting
- Anorexia
In detail; There are marked individual differences in presentation of withdrawal symptoms. Additionally, Heroin withdrawal syndrome is far more severe than the withdrawal syndrome seen with morphine. [2]
Complications
Biological:
Infections e.g.:
- Abscesses and cellulitis
- Sepsis
- HIV
- Hepatitis B or C
- Bacterial endocarditis
Cardiorespiratory e.g.:
- Deep vein thrombosis or embolism
- Aspiration
- Respiratory depression
- Cardiac arrhythmias
Complications of pregnancy
Death from overdose
Psychological:
- Depression
- Anxiety disorders
- Deliberate self-harm
- Suicide
Social:
- Unemployment
- Loss of accommodation
- Breakdown of relationships
- Loss of friends
- Criminal record [1]
Investigations
Tab Content
Treatment
The treatment can be divided into three main types:
1. Firstly; Treatment of overdose.
2. Secondly; Detoxification.
3. Thirdly; Maintenance therapy.
1. Treatment of Opioid Overdose:
The key clinical findings in a patient who has taken an overdose of opioids are:
- Respiratory depression (rate less than eight breaths per minute), possibly leading to respiratory arrest
- Unreactive pinpoint pupils
- Bradycardia
- Hypotension
- Snoring or other upper airway sounds
- Reduced level of consciousness.
Patients should be approached using the principles of airway, breathing, also circulation and treated with oxygen, respiratory support, fluids, and inotropes if necessary. [1]
An overdose of opioid can treated with narcotic antagonists (such as naloxone, naltrexone). Additionally; Usually an intravenous injection of 2 mg naloxone, followed by a repeat injection in 5-10 minutes, can cause reversal of overdose.
But as naloxone has a short half-life repeated doses may be needed every 1-2 hours. Lastly; This should combined with general care and supportive treatment. [2]
2. Detoxification (Planned withdrawal of opioids):
This is a mode of treatment in which the dependent person is ‘taken off’ opioids. In detail; This is usually done abruptly, followed by management of emergent withdrawal symptoms.
It is highly recommend that detoxification is conduct in a safe manner under expert guidance of a specialist.
The withdrawal symptoms can managed by one of the following methods i.e.:
Use of substitution drugs i.e.:
Such as methadone to ameliorate the withdrawal symptoms. The aim is to gradually taper off the patient from methadone (which is less addicting, has a longer half-life, decreases possible criminal behaviour, and has a much milder withdrawal syndrome).
However, relapses are common and its opponents argue that one type of dependence is often replaced by another (methadone).
Clonidine i.e.:
Basically; It is an α2 agonist that acts by inhibiting norepinephrine release at presynaptic α2 receptors. The usual dose is 0.3-1.2 mg/day, also drug is tapered off in 10-14 days.
It can be started after stoppage of either the opioid itself or the substitution drug (for example; methadone). The important side effects of clonidine are excessive sedation and postural hypotension.
Lastly; Clonidine treatment is usually started in an inpatient psychiatric or specialist alcohol and drug treatment center setting.
Naltrexone with Clonidine i.e.:
Naltrexone is an orally available narcotic antagonist which, when give to an opioid dependent individual, causes withdrawal symptoms. These symptoms are manage with the addition of clonidine for 10-14 days after which clonidine is withdraw and the patient is continue on naltrexone alone.
Now if the person takes an opioid, there are no pleasurable experiences, as the opioid receptors are block by naltrexone.
Therefore, this method is a combination of detoxification and maintenance treatment. The usual dose of naltrexone is 100 mg orally, administered on alternate days.
Other Drugs i.e.:
The other detoxification agents include LAAM (levo-alpha-acetyl-methadol), propoxyphene, diphenoxylate, buprenorphine (long acting synthetic partial μ-agonist which can be administered sublingually), and lofexidine (α2 agonist, similar to clonidine).
In particular, Buprenorphine has recently used widely for detoxification as well as for maintenance treatment in many parts of the World. Care must be exercised as there is potential for misuse with buprenorphine. [2]
When heroin is withdrawn, psychological support is particularly important to avoid immediate relapse. Withdrawal usually undertaken by substituting methadone (a longer-acting drug) for heroin.[1]
3. Maintenance Therapy:
After the detoxification phase is over, the patient is maintain on one of the following regimens:
Methadone maintenance (Agonist substitution therapy) i.e.:
This a very popular method use widely in the Western World. 20-50 mg/day of methadone is give to the patients to ‘shift’ them from ‘hard’ drugs, thus decreasing IV use and criminal behaviour.
Its use in India has not recommended by an expert committee for de-addiction services. Other drugs such as LAAM and buprenorphine can used for maintenance treatment.
Opioid antagonists i.e.:
Opioid antagonists have in use for a long time but they were either partial antagonists (such as n alorphine) or had to administer parenterally (such as naloxone).
Furthermore; The usual maintenance dose is 100 mg on Mondays and Wednesdays, and 150 mg on Fridays.
Naltrexone combine with clonidine, as describe above, is a very effective method for detoxification as well as for maintenance treatment.
Other methods i.e.:
These include individual psychotherapy, behaviour therapy, interpersonal therapy, cognitive behaviour therapy (CBT), motivational enhancement therapy, self-control strategies, psychotropic drugs for associated psychopathology, family therapy, and group therapy (e.g. in therapeutic communities such as Synanon, self-help groups such as Narcotic Anonymous or NA).
These methods have to tailored for use in an individual patient.
Psychosocial rehabilitation i.e.:
This is a very important step in the post-detoxification phase, in the absence of which relapse rates can very high. Rehabilitation should at both occupational and social levels. [2]
Prevention
Tab Content
Homeopathic Treatment
Diet & Regimen
Do’s and Dont’s
Tab Content
Terminology
Tab Content
References
- Psychiatry, Fourth Edition- Oxford Medical Publications – SRG- by Geddes, Jonathan Price, Rebecca McKnight / Ch 29.
- A Short Textbook of Psychiatry by Niraj Ahuja / Ch 4
FAQ
Frequently Asked Questions
What is Opioid Use Disorder?
Opioids are substances that mimic the effects of endogenous opioids (endorphins and enkephalins) by acting as agonists at the opioid receptors.
Name of the derivatives of Opioid?
- Morphine
- Codeine
- Thebaine
- Noscapine
- Papaverine
- Heroin
- Nalorphine
- Hydromorphone
- Methadone
What is Acute Intoxication of Opioid Use Disorder?
- Apathy
- Bradycardia
- Hypotension
- Respiratory depression
- Subnormal core body temperature
- Pin-point pupils
What is Withdrawal Syndrome of Opioid Use Disorder?
Also Search As
Frequently Asked Questions (FAQ)
XYZ
XXX
XYZ
XXX
XYZ
XXX
How can I find reputable homeopathy clinics or homeopathic doctors in my area?
You can found Homeopathic Clinic For XXXX by searching for
Specific city Examples are
You can also search for near you Examples are