Personality Disorders:
Definition:
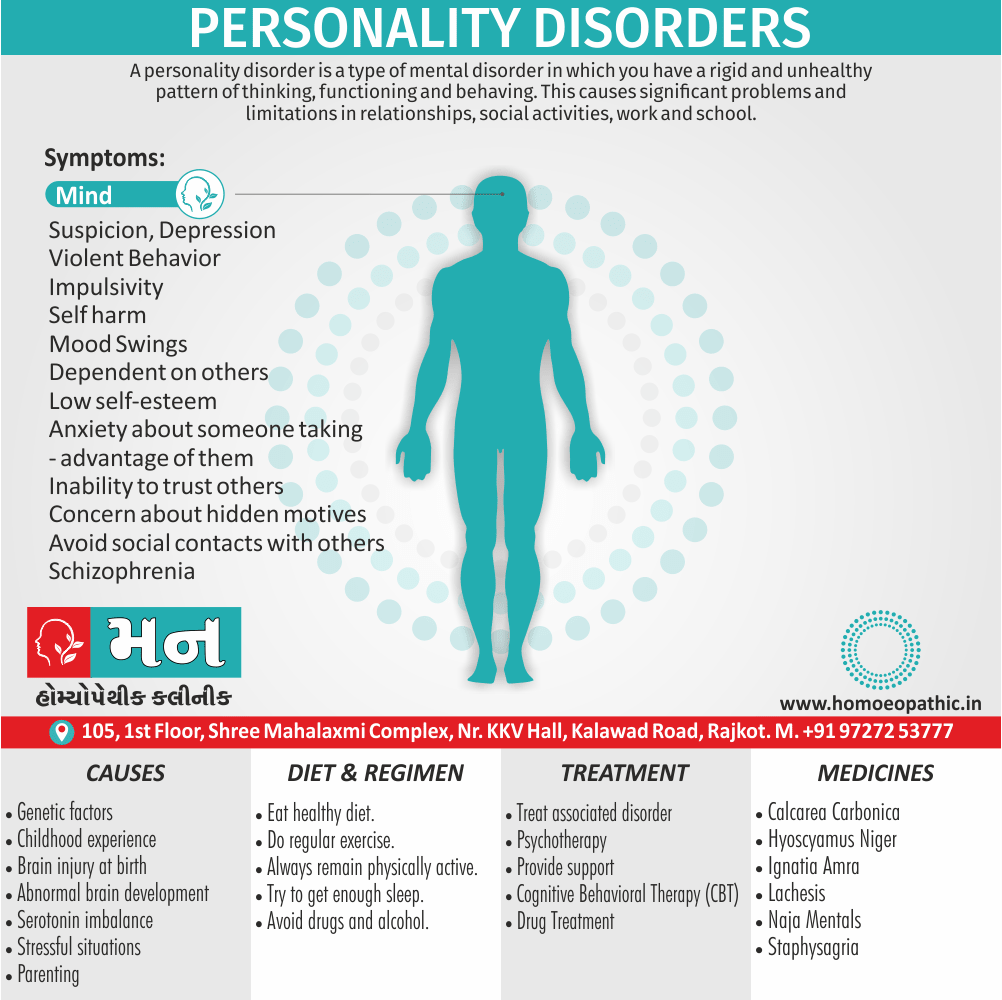
A personality disorders is a type of mental disorder in which you have a rigid and unhealthy pattern of thinking, functioning and behaving. A person with a personality disorder has trouble perceiving and relating to situations and people. This causes significant problems and limitations in relationships, social activities, work and school.
Personality disorder:
When the behaviour is inflexible, maladaptive, and antisocial, then the individual is diagnosed with a personality disorder.
In some cases, you may not realize that you have a personality disorder because your way of thinking and behaving seems natural to you. And you may blame others for the challenges you face.
Personality disorders usually begin in the teenage years or early adulthood. sometimes even childhood and often have a pervasive negative impact on the quality of life .
There are many types of personality disorders. Some types may become less obvious throughout middle age.
People with a personality disorder may:
React in unusual ways to illness or to treatment; for example, by becoming overdependent or aggressive;
Behave in unusual ways when mentally ill, so that diagnosis is difficult;
React unusually to stressful events; for example, by becoming aggressive or histrionic instead of anxious; sometimes these reactions are so unusual that they may be mistaken for a psychiatric disorder;
Behave in ways that are stressful or dangerous to themselves or other people;
Develop other psychiatric disorders more often than other people.
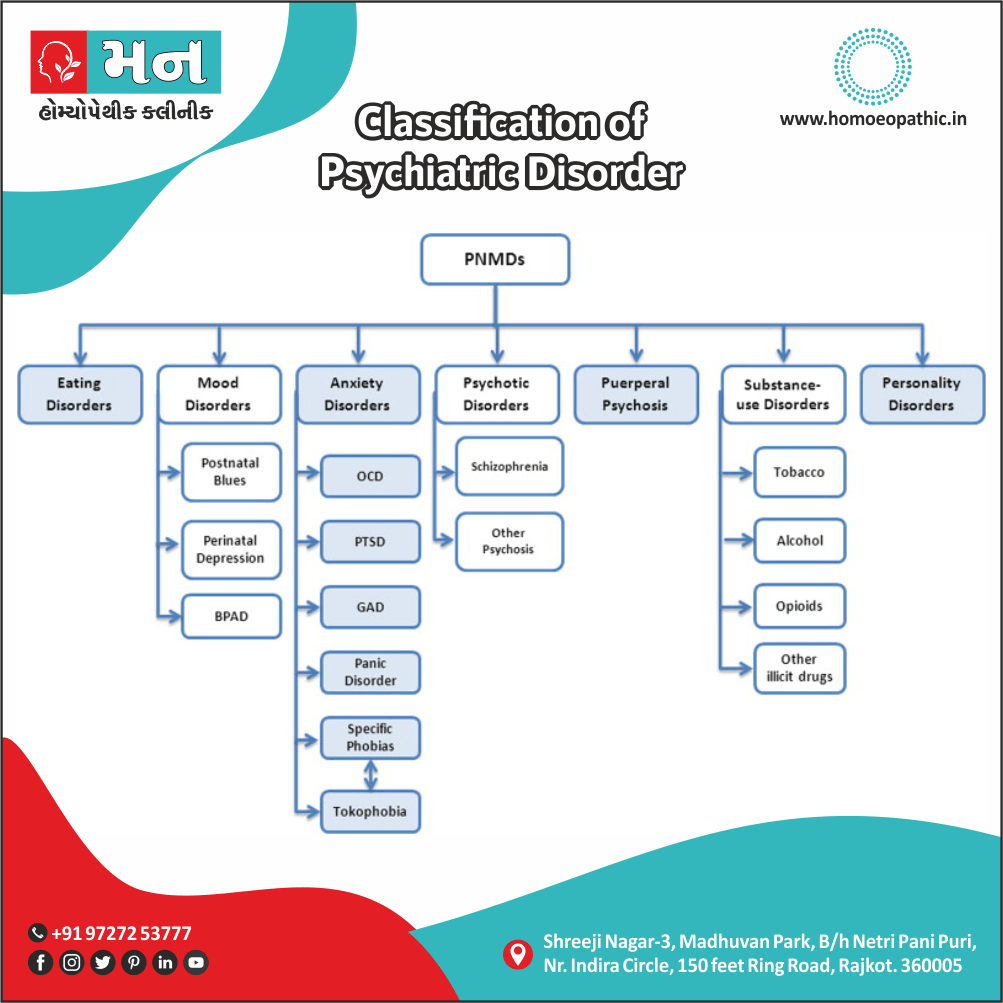
Types
Psychiatrists classify abnormal personalities according to one or other of the detailed schemes set out in ICD-10 and DSM-IV.
For other doctors, who treat people with highly abnormal personalities less often, a simpler scheme is usually adequate.
Such a scheme is compatible with the specialist classifications (with one exception— lacking self-esteem). Each of the groups in this scheme will be described together with its relationship to the specialist classification, which is shown below.
Note that:
- the category for personalities lacking self-esteem and self confidence is included in neither DSM-IV nor ICD-10;
- cyclothymic and schizotypal ‘personalities’ are not included in the classification of personality disorder, but in ‘two minds mood disorder’ and ‘schizophrenia’, respectively, due to their close epidemiological links to those disorders.
A simplified classification of personality:
- Anxious, moody, and prone to worry
- Lacking self-esteem and confidence
- Sensitive and suspicious
- Dramatic and impulsive
- Aggressive and antisocial
Classification of personality disorders in DSM-IV and ICD-10 (generally, the same terms are used in DSM-IV and ICD-10; where there are differences the ICD term is shown in parentheses):
-
Anxious, moody, and prone to worry e.g.:
- Avoidant (anxious)
- Obsessive-compulsive (anankastic)
- Dependent
- Affective (depressive, hyperthymic, cyclothymic)
-
Sensitive and suspicious e.g.:
- unreasonable
- Schizoid
- Schizotypal (ICD-10: classified with schizophrenia)
-
Dramatic and impulsive e.g.:
- Histrionic
- Borderline (emotionally unstable—impulsive)
- self-centered
-
Antisocial e.g.:
- Antisocial (dissocial)
1.Anxious, Moody and Prone to Worry Personalities:
(i) Avoidant (anxious) personality disorder i.e.:
These people are persistently anxious, ill at ease in company, and fearful of disapproval or criticism. They feel inadequate and are timid. They avoid taking new responsibilities at work and avoid new experiences generally. This tendency to avoid is the basis of the DSM term avoidant.
Characteristics of anxious, moody, worry-prone personalities i.e.:
- Persistently anxious
- Worried about day-to-day problems or health
- Inflexible, obstinate, indecisive (obsessional traits)
- Persistently gloomy and pessimistic or
- Unstable moods, mild elation, or overconfidence alternates with mild depression and/or selfdeprecation
(ii) Obsessive-compulsive (anankastic) personality disorder:
These people are inflexible, obstinate, and rigid in their opinions, and they focus on unimportant detail. They are indecisive, and having made a decision they worry about its consequences.
They are humourless and judgemental, while worrying about the opinions of others. Perfectionism, rigidity, and indecisiveness can make employment impossible.
They appear outwardly controlled but may well be irritated by those who disturb their carefully ordered routine, and may have violent feelings of anger.
(iii) Dependent personality disorder:
These people are passive and unduly compliant with the wishes of others. They lack vigour and self-reliance, and they avoid responsibility. Some achieve their aims by persuading other people to assist them, while protesting their own helplessness.
Some are supported by a more self- reliant partner; left to themselves, they have difficulty in dealing with the demands and also responsibilities of everyday life.
(iv) Persistent mood disorders:
These disorders represent a lifelong tendency to persistent gloom, elation, or varied mood which is abnormal, but not severe enough at any one time to constitute depressive or wild episodes.
Because of the close epidemiological links that we now know exist between these disorders and the mood (affective) disorders, the ‘affective personality disorders’ are now classified among the mood disorders in both DSM-IV and ICD-10. These people have lifelong abnormalities of mood regulation, as follows:
a.Dysthymia (ICD-10 and DSM-IV): Formerly depressive personality disorder. The person is persistently gloomy and pessimistic with little capacity for enjoyment.
b.Cyclothymia (ICD-10 and DSM-IV): Formerly cyclothymic personality disorder. The person’s mood alternates between gloomy and elated over periods of days to weeks. This instability can be particularly disruptive to work and social relationships.
2.Personalities lacking Self esteem and Confidence:
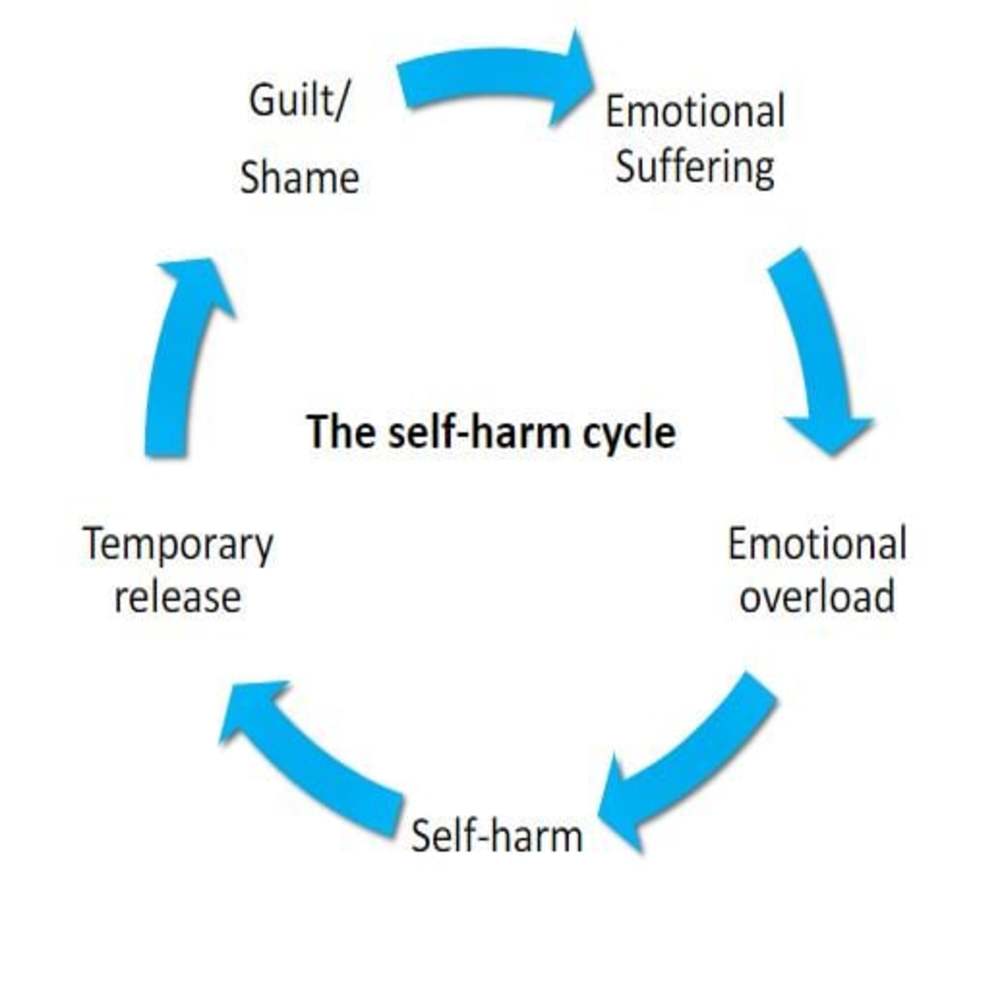
This group is common and important in primary care and general medical practice. These personality features are associate with recurrent depressive moods, eating disorders, and self-harm and are often see among young people who seek help for these problems.
Unfortunately, this group does not appear as a separate entity in the specialist classifications of personality disorder.
Characteristics of personalities lacking self-esteem:
- Lack confidence
- Feel inferior
- Expect criticism
- Strive to please others
- Shyness and social withdrawal/inappropriate efforts to please others
3.Sensitive and Suspicious Personalities:
People in this group are difficult to engage in treatment and they may distrust their doctors:
Characteristics of sensitive and suspicious personalities:
- Sensitive, touchy, irritable; see rebuffs where none exist
- Suspicious, mistrustful
- Cold, detached,show little concern for others,reject help when it is offered
- Eccentric, with unusual ideas about topics such as telepathy
- Self-sufficient
- Lacking concern
(i) Paranoids personality disorder:
These individuals are sensitive and suspicious; they mistrust others and suspect their motives, and are prone to jealousy. They are touchy, irritable, argumentative, and stubborn.
Some of these people have a strong sense of self-importance and special ability, although they may feel that their potential has been stymied by others letting them down or deceiving them.
(ii) Schizoid personality disorder:
These individuals are emotionally cold, self-sufficient, and detached. They are introspective and may have a complex fantasy life.
They show little concern for the opinions of others, and pursue a solitary course through life. When this personality disorder is extreme, the person is cold, callous, and insensitive.
(iii) Schizotypal personality disorder:
These individuals are eccentric and have unusual ideas (e.g. about telepathy and clairvoyance) or ideas of reference. Their speech is abstract and vague, and their affect may be inappropriate to the circumstances. In ICD-10
4.Dramatic and Impulsive Personalities:
characteristics of dramatic and impulsive personalities:
- Seek the limelight, dramatize their problems
- Vain, self-centered
- Demanding of others, to an unreasonable extent, perhaps using ‘emotional blackmail’
- Act a part, self-deceiving, lack awareness of their image to others
- Impulsive, sometimes with harmful behaviours
- Short-lived enthusiasms but lack persistence
- Unrestrained emotional display
(i) Borderline personality disorder:
People with borderline personality represent an important clinical group that presents frequently to healthcare, including A&E departments.
The term ‘borderline’ refers to a combination of features seen also in histrionic and antisocial personalities, which are centred around impulsivity and poor self-control.
The term originates in the now abandoned idea that the condition was related to (on the borderline with) schizophrenia.
Note that ICD-10 uses the term emotionally unstable personality disorder for the same patient group. People with borderline personality disorder have intense but unstable relationships.
They have persistent feelings of boredom and emptiness, with uncertainty about personal identity and a fear of abandonment. Their moods may be unstable, with unwarranted outbursts of anger, and low tolerance of stress.
They are impulsive, and may engage in self damaging behaviours, such as reckless spending or gambling, reckless sex, chaotic eating, and substance abuse. Threats or acts of self-harm may be recurrent.
(ii) Histrionic personality disorder:
These people appear sociable, outgoing, and entertaining but at the same time they are self-centred, prone to short lived enthusiasms, and lack persistence.
Extreme displays of emotion may leave others exhausted while the person recovers quickly and without remorse. Sexually provocative behaviour is common but tender feelings are lacking.
There may be astonishing capacity for self-deception and an ability to persist with elaborate lies long after others have seen the truth.
(iii) self-centered personality disorder:
This disorder is not included in ICD-10. Narcissism is morbid self-admiration. self-centered people have a grandiose sense of self-importance and are preoccupied with fantasies of success, power, and intellectual brilliance.
They crave attention, exploit others, and seek favours but do not return them.
5.Antisocial Personality:
This group corresponds to the dissocial (ICD-10) or antisocial (DSM-IV) groups in the specialist classifications. The difficulties are often increased by abuse of alcohol or illicit drugs.
Characteristics of antisocial personalities:
- Impulsive behaviour, low tolerance of frustration, and lack of consistent striving towards goals, leading to, for example, an unstable work record
- Callous acts, inflicting pain, cruelty, or degradation on others
- Tendency to violence
- Lack of guilt
- Failure to learn from experience, leading to behaviours that persist or escalate despite negative social consequences and legal penalties
- Failure to sustain close relationships, including intimate relationships
- Disregard of the feelings of others
- Family problems, including violence towards partner, and neglect of or violence towards children; frequent separation and divorce
- Often lengthy forensic history, perhaps starting with petty delinquent acts but escalating to callous, violent crime.
Personality is the combination of thoughts, emotions and behaviors that makes you unique. It’s the way you view, understand and relate to the outside world, as well as how you see yourself.
Personality forms during childhood, shaped through an interaction of:
Genetic factors:
The children of parents with antisocial personality disorder have greater rates of antisocial behaviour than children of parents who do not have this personality.
A similar excess has been reported also among adopted children whose biological parents have antisocial personality disorder and whose adoptive parents do not. These findings suggest a genetic contribution to aetiology.
Childhood experience:
Separation from parents in early childhood is more frequent among people with antisocial personality disorder than among controls.
This association could be due to
(i) Firstly, parental disharmony preceding separation,
(ii) Secondly, the separation itself, or
(iii) Thirdly, a consequence of separation such as upbringing in care rather than in a family.
Injury to the brain at birth:
It is sometimes followed by impulsive and aggressive behaviour. Such injury has been suggested as a cause of antisocial personality disorder but without convincing evidence.
Abnormal brain development:
It has been suggested as a cause. The only evidence, which is indirect, is that some adults with antisocial personality have non-specific features in the electroencephalogram (EEG) of a kind found normally in adolescents, not adults.
This suggests that these findings might reflect delayed brain maturation among people with antisocial personality.
Serotonin:
Recent studies have found an association between aggressive behaviour and low levels of brain serotonin (5-HT), inferred from the results of neuroendocrine challenge tests.
However, the association between serotonin and aggression is not confined to aggression in antisocial personality disorder.
Parenting:
Evidence shows personality disorders may begin with parental personality issues. These cause the parent to have their own difficulties in adulthood, such as difficulties reaching higher education, obtaining jobs, and securing dependable relationships.
By either genetic or modeling mechanisms, children can pick up these traits.
More specifically, lack of maternal bonding has also been correlated with personality disorders. In a study comparing 100 healthy individuals to 100 borderline personality disorder patients, analysis showed that BPD patients were significantly more likely not to have been breastfed as a baby.
These researchers suggested this act may be essential in fostering maternal relationships.
Negative correlation
Additionally, findings suggest personality disorders show a negative correlation with two attachment variables: maternal availability and dependability.
When left unfostered, other attachment and interpersonal problems occur later in life ultimately leading to development of personality disorders.
Personality disorders are thought to be caused by a combination of these genetic and environmental influences.
Your genes may make you vulnerable to developing a personality disorder, and a life situation may trigger the actual development.
By definition, personality is enduring and stable. Small changes often take place very gradually over many years; for example, a person may become less impulsive and aggressive in middle or late life, or a person who is socially anxious and lacking in confidence in their 20s becomes socially and occupationally adept in their 30s and 40s.
The term personality change does not refer to these gradual modifications but to the more abrupt, step-like changes that result sometimes from:
- Injury to, or organic disease of, the brain;
- Residual effects of severe mental disorder, usually schizophrenia;
- Exceptionally severe stressful experiences such as those experienced by hostages or victims of severe torture.
Sources of information:
In everyday life we learn about the personalities of people we know by observing how they respond in various circumstances over the time that we have known them. There are four sources of information:
- A description by someone who knows the patient well, a corroborant. If that person is observant and reliable, this is usually the best source.
- The patient’s own account of their past behaviour in a variety of circumstances. It is less objective but potentially more complete.
- A patient’s own account of their personality. This is also subjective and sometimes influenced by the wish to create a good impression, or by depression or elation.
- The patient’s behaviour in the interview. It is often unreliable because it reflects their current mood and the context of the interview.
The evaluation of personality formed from the last two of these items should be checked by comparing it with an objective record of past achievements and difficulties and, whenever possible, with the accounts of people who know the patient well.
A scheme for assessing personality:
1.Relationships:
This section is concerned with (i) relationships at work (with colleagues, people in authority, and juniors), (ii) relationships with friends, and (iii) intimate relationships.
The interviewer asks whether the patient makes friends easily, has few friends or many, has close friends in whom they can confide, and has lasting friendships. The interviewer also asks whether the patient is sociable and confident in company, or shy and reserved.
Finally, ask about the nature of romantic relationships—their nature, quality, and sense of permanence or instability.
2.Usual mood:
The aim is to discover the person’s usual or habitual mood, not the present or recent mood. There are three elements.
(i) the general character of the person’s mood; is it generally cheerful, middle of the road, or gloomy?
(ii) whether it is stable, changeable, or volatile. If mood is changeable, the interviewer asks how long the changes last, and whether they occur spontaneously or in relation to events.
(iii) whether the person shows his feelings or hides them.
Other traits:
When enquirer about other traits it can help to keep in mind the list which is given below; Each characteristic has a positive as well as a negative side and it is appropriate to ask patients where they lie between the extremes;
Common personality traits (for brevity, only negative attributes are listed; corresponding positive features should also be noted):
- Prone to worry ● Impulsive
- Strict, fussy, rigid ● Attention seeking
- Lacking self-confidence ● Dependent
- Sensitive ● Aggressive
- Suspicious, jealous ● Irritable, quarrelsome
- Untrusting, resentful ● Lacking concern for others
It is useful to check answers by asking for examples from the patient’s recent life, and checking with a corroborant.
Characteristics such as jealousy or lack of feeling for others may not be revealed because the person is ashamed of them or does not recognize their presence.
Observations should be recorded objectively, avoiding value judgements. General terms such as ‘immature’ or ‘inadequate’ should not be used; instead, the interviewer should record in what ways the person has difficulty in meeting the demands of adult life.
4.Attitudes, beliefs, and standards:
Relevant points include attitudes to illness, religious beliefs, and personal standards. Usually, these become apparent when the personal history is being taken, but they can be explored further at this point in the interview.
Usual habits:
Although not strictly part of personality, the person’s usual lifestyle is often relevant. What was their typical daily routine (timeline, structure, activities), and what was their typical daily use of tobacco, alcohol, and illicit drugs?
These aspects of a person’s life may help by (i) indicating possible aetiological factors in current mental illness, or (ii) indicating possible features of current mental illness.
For example, a person whose usual alcohol habit was to drink half a bottle of wine on a Friday and Saturday evening with friends may start to drink more than half a bottle each evening on their own, as ‘self-medication’ to cope with their low mood.
If your doctor suspects you have a personality disorder, a diagnosis may be determined by:
- Physical exam. The doctor may do a physical exam and ask in-depth questions about your health. In some cases, your symptoms may link to an underlying physical health problem. Your evaluation may include lab tests and a screening test for alcohol also drugs.
- Psychiatric evaluation. This includes a discussion about your thoughts, feelings and behavior and may include a questionnaire to help pinpoint a diagnosis. Additionally, With your permission, information from family members or others may be helpful.
- Diagnostic criteria in the DSM-5. Your doctor may compare your symptoms to the criteria in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published by the American Psychiatric Association.
Diagnostic criteria:
Each personality disorder has its own set of diagnostic criteria.
However, according to the DSM-5, generally the diagnosis of a personality disorder includes long-term marked deviation from cultural expectations that leads to significant distress or impairment in at least two of these areas:
- The way you perceive and interpret yourself, other people and events
- The appropriateness of your emotional responses
- How well you function when dealing with other people and in relationships
- Whether you can control your impulses
Furthermore, sometimes it can be difficult to determine the type of personality disorder, as some personality disorders share similar symptoms and more than one type may present.
Aims of management
-
Identify and treat any co-morbid psychiatric disorders.
For example: Depression should consider whenever the personality problems have increased recently without another obvious cause, even when the patient does not complain spontaneously of depression.
-
Treat any associated substance misuse.
Alcohol or other substances may use by people with personality disorder to relieve tension, unhappiness, or feelings of inadequacy. However, they can exacerbate mood disturbance, and their disinhibiting effects can encourage histrionic or aggressive behaviour and self-harm.
-
Help the patient to deal with or avoid situations that provoke problem behaviours.
for problem behaviours by asking the patient to keep a daily diary of the behaviours and the situations in which they occur. For example, aggression may be provoked by social rejection, which is the response of others to the patient’s lack of social skills. Treatment would then include social skills training.
-
Provide general support to reduce tension and increase self-esteem.
particularly the effects on any children living with the patient. Although these enquiries are particularly important when the person is aggressive, the problems of people who are persistently anxious, histrionic, or suspicious may also affect their families.
-
Support and help the family.
This may be needed especially when the personality disorder is of the aggressive or antisocial kind. If a mother has a personality disorder, the health and development of the children should assesse, and appropriate steps taken to alleviate any problems.
Psychotherapy:
During psychotherapy with a mental health professional, you can learn about your condition and talk about your moods, feelings, thoughts and behaviors. You can learn to cope with stress and manage your disorder.
First of all, Psychotherapy may be provided in individual sessions, group therapy, or sessions that include family or even friends. There are several types of psychotherapy — your mental health professional can determine which one is best for you.
You may also receive social skills training. During this training you can use the insight and knowledge you gain to learn healthy ways to manage your symptoms and reduce behaviors that interfere with your functioning and relationships.
Family therapy provides support and education to families dealing with a family member who has a personality disorder.
Medications:
There are no medications specifically approved by the Food and Drug Administration (FDA) to treat personality disorders. However, several types of psychiatric medications may help with various personality disorder symptoms.
- Antidepressants. Antidepressants such as the SSRI fluoxetine, may be useful if you have a depressed mood, anger, impulsivity, irritability or hopelessness, which may be associated with borderline personality disorders.
- Mood stabilizers. Such as lithium carbonate and other anticonvulsants are useful. Additionally, As their name suggests, mood stabilizers can help even out either mood swings or reduce irritability, impulsivity and aggression.
- Antipsychotic medications. Also called neuroleptics, these may be helpful if your symptoms include losing touch with reality (psychosis) or in some cases if you have either anxiety or anger problems.
- Anti-anxiety medications. These may help if you have anxiety, agitation or insomnia. But in some cases, they can increase impulsive behavior, so they’re avoided in certain types of personality disorders.
Useful Remedies:
Calcarea carbonica:
This remedy is usually indicated for dependable solid people who become overwhelmed from physical illness or too much work and start to fear a breakdown.Their thoughts can be muddled and confused when tired, which adds to the anxiety. Worry may agitate them, and a nagging dread of disaster (to themselves or others) may develop. Fear of heights and claustrophobia are also common. A person who needs this remedy is often chilly and sluggish, has a craving for sweets, and is easily fatigued.
Ignatia Amara:
A sensitive person who is anxious because of grief, loss, disappointment, criticism, loneliness (or any stressful emotional experience) may benefit from this remedy. A defensive attitude, frequent sighing, and mood swings are other indications. The person may burst unexpectedly into either tears or laughter. Headaches that feel like a nail driven into the side of the head, and cramping pains in the abdomen or back, are often seen when this remedy is needed.
Naja mentals:
Sense of duality the feeling of being split into two, of having two wills. Conflict between higher (human) and lower (animal) nature, strong sense of duty (which in the duality-neglect), feels as if he is a failure. Delusion he has suffered-broods over imaginary troubles (which in the duality suffering wrong and doing wrong to others). Timidity fear of rain, fear of being abandoned.
Keynotes:
Affinities: Cerebellum, Medulla, Nerves, Heart, respiration- throat. Worse: specifically lying on left side. After sleep, after menses. Air (cold; drafts) Damp Weather. Tight clothing. Alcohol. Exertion. Talking. Walking. Night. Touch. 3 pm. Stimulants. On the other hand, Better: Walking and riding in open air. Sneezing. Lying on right side. Very sensitive to cold- desires warmth. Colds that turn to asthma. Sensation as if organs are drawn together.
Some other remedies, which can be used in these cases are:
apis, hyoscyamus, lachesis, cannabis sativa, spongia, aurum met, derris pin- nata, opium, agaricus, bovista, staphysagria, meliotus, tellurium, gelse- mium, bryonia, etc.
Lifestyle and home remedies:
Along with your professional treatment plan, consider these lifestyle and self-care strategies:
Be an active participant in your care.
Generally, This can help your efforts to manage your personality disorder. Don’t skip therapy sessions, even if you don’t feel like going. Think about your goals for treatment and work toward achieving them.
Take your medications as directed.
Even if you’re feeling well, don’t skip your medications. If you stop, symptoms may come back. Additionally, You could also experience withdrawal-like symptoms from stopping a medication too suddenly.
Learn about your condition.
In brief, Education about your condition can empower you and motivate you to stick to your treatment plan.
Get active.
Physical activity can help manage many symptoms, such as depression, stress and anxiety. It can also counteract the effects of some psychiatric medications that may cause weight gain. Consider walking, jogging, swimming, gardening or taking up another form of physical activity that you enjoy.
Avoid drugs and alcohol.
Alcohol also street drugs can worsen personality disorder symptoms or interact with medications.
Get routine medical care.
Don’t neglect checkups or skip visits to your primary care professional, especially if you aren’t feeling well. You may have a new health problem that needs to address, or you may be experiencing side effects of medication.
Caring and support:
Having a personality disorder makes it hard to engage in behavior and activities that may help you feel better. In detail, Ask your doctor or therapist how to improve your coping skills and get the support you need.
Furthermore, If you have a loved one with a personality disorder, work with his or her mental health professional to find out how you can most effectively offer support and encouragement.
You may also benefit from talking with a mental health professional about any distress you experience.
All in all, A mental health professional can also help you develop boundaries and self-care strategies so that you’re able to enjoy and succeed in your own life.
Frequently Asked Questions
What is Personality Disorders?
A personality disorder is a type of mental disorder in which you have a rigid and unhealthy pattern of thinking, functioning and behaving.
Homeopathic Medicines used by Homeopathic Doctors in treatment of Personality Disorders?
- Calcarea carbonica
- Ignatia Amara
- Naja
- Apis
- Hyoscyamus
- Lachesis
What causes Personality Disorders?
- Genetic factors
- Childhood experience
- Injury to the brain at birth
- Abnormal brain development
- Serotonin
- Parenting
What are the symptoms of Personality Disorders?
A person may become less impulsive and aggressive in middle or late life, or a person who is socially anxious and lacking in confidence in their 20s becomes socially and occupationally adept in their 30s and 40s.
Give the types of ?
- Anxious, moody, and prone to worry
- Lacking self-esteem and confidence
- Sensitive and suspicious
- Dramatic and impulsive
- Aggressive and antisocial
Definition:
Definition:
A personality disorders is a type of mental disorder in which you have a rigid and unhealthy pattern of thinking, functioning and behaving. A person with a personality disorder has trouble perceiving and relating to situations and people. This causes significant problems and limitations in relationships, social activities, work and school.
Overview
Epidemiology
Causes
Risk Factors
Pathogenesis
Pathophysiology
Types
Personality Change
Assessment of Personality
Clinical Features
Sign & Symptoms
Clinical Examination
Diagnosis
Differential Diagnosis
Complications
Investigations
Treatment
Prevention
Homeopathic Treatment
Diet & Regimen
Lifestyle and Home Remedies
Do’s and Dont’s
Terminology
References
FAQ
Also Search As
Overview
Personality disorder:
When the behaviour is inflexible, maladaptive, and antisocial, then the individual is diagnosed with a personality disorder.
In some cases, you may not realize that you have a personality disorder because your way of thinking and behaving seems natural to you. And you may blame others for the challenges you face.
Personality disorders usually begin in the teenage years or early adulthood. sometimes even childhood and often have a pervasive negative impact on the quality of life .
There are many types of personality disorders. Some types may become less obvious throughout middle age.
People with a personality disorder may:
React in unusual ways to illness or to treatment; for example, by becoming overdependent or aggressive;
Behave in unusual ways when mentally ill, so that diagnosis is difficult;
React unusually to stressful events; for example, by becoming aggressive or histrionic instead of anxious; sometimes these reactions are so unusual that they may be mistaken for a psychiatric disorder;
Behave in ways that are stressful or dangerous to themselves or other people;
Develop other psychiatric disorders more often than other people.
Epidemiology
Indian epidemiology then other
Causes
Personality is the combination of thoughts, emotions and behaviors that makes you unique. It’s the way you view, understand and relate to the outside world, as well as how you see yourself.
Personality forms during childhood, shaped through an interaction of:
Genetic factors:
The children of parents with antisocial personality disorder have greater rates of antisocial behaviour than children of parents who do not have this personality.
A similar excess has been reported also among adopted children whose biological parents have antisocial personality disorder and whose adoptive parents do not. These findings suggest a genetic contribution to aetiology.
Childhood experience:
Separation from parents in early childhood is more frequent among people with antisocial personality disorder than among controls.
This association could be due to
(i) Firstly, parental disharmony preceding separation,
(ii) Secondly, the separation itself, or
(iii) Thirdly, a consequence of separation such as upbringing in care rather than in a family.
Injury to the brain at birth:
It is sometimes followed by impulsive and aggressive behaviour. Such injury has been suggested as a cause of antisocial personality disorder but without convincing evidence.
Abnormal brain development:
It has been suggested as a cause. The only evidence, which is indirect, is that some adults with antisocial personality have non-specific features in the electroencephalogram (EEG) of a kind found normally in adolescents, not adults.
This suggests that these findings might reflect delayed brain maturation among people with antisocial personality.
Serotonin:
Recent studies have found an association between aggressive behaviour and low levels of brain serotonin (5-HT), inferred from the results of neuroendocrine challenge tests.
However, the association between serotonin and aggression is not confined to aggression in antisocial personality disorder.
Parenting:
Evidence shows personality disorders may begin with parental personality issues. These cause the parent to have their own difficulties in adulthood, such as difficulties reaching higher education, obtaining jobs, and securing dependable relationships.
By either genetic or modeling mechanisms, children can pick up these traits.
More specifically, lack of maternal bonding has also been correlated with personality disorders. In a study comparing 100 healthy individuals to 100 borderline personality disorder patients, analysis showed that BPD patients were significantly more likely not to have been breastfed as a baby.
These researchers suggested this act may be essential in fostering maternal relationships.
Negative correlation
Additionally, findings suggest personality disorders show a negative correlation with two attachment variables: maternal availability and dependability.
When left unfostered, other attachment and interpersonal problems occur later in life ultimately leading to development of personality disorders.
Personality disorders are thought to be caused by a combination of these genetic and environmental influences.
Your genes may make you vulnerable to developing a personality disorder, and a life situation may trigger the actual development.
Risk Factors
Risk factors are things that make you more likely to develop a disease in the first place.
Pathogenesis
Pathogenesis refers to the development of a disease. It’s the story of how a disease gets started and progresses.
This is the entire journey of a disease, encompassing the cause but going beyond it.
Pathophysiology
Pathophysiology, on the other hand, focuses on the functional changes that occur in the body due to the disease. It explains how the disease disrupts normal physiological processes and how this disruption leads to the signs and symptoms we see.
Imagine a car accident. Pathogenesis would be like understanding how the accident happened – what caused it, the sequence of events (e.g., one car ran a red light, then hit another car). Pathophysiology would be like understanding the damage caused by the accident – the bent fenders, deployed airbags, and any injuries to the passengers.
In simpler terms, pathogenesis is about the "why" of a disease, while pathophysiology is about the "how" of the disease’s effects.
Types
Types
Psychiatrists classify abnormal personalities according to one or other of the detailed schemes set out in ICD-10 and DSM-IV.
For other doctors, who treat people with highly abnormal personalities less often, a simpler scheme is usually adequate.
Such a scheme is compatible with the specialist classifications (with one exception— lacking self-esteem). Each of the groups in this scheme will be described together with its relationship to the specialist classification, which is shown below.
Note that:
- the category for personalities lacking self-esteem and self confidence is included in neither DSM-IV nor ICD-10;
- cyclothymic and schizotypal ‘personalities’ are not included in the classification of personality disorder, but in ‘two minds mood disorder’ and ‘schizophrenia’, respectively, due to their close epidemiological links to those disorders.
A simplified classification of personality:
- Anxious, moody, and prone to worry
- Lacking self-esteem and confidence
- Sensitive and suspicious
- Dramatic and impulsive
- Aggressive and antisocial
Classification of personality disorders in DSM-IV and ICD-10 (generally, the same terms are used in DSM-IV and ICD-10; where there are differences the ICD term is shown in parentheses):
Anxious, moody, and prone to worry e.g.:
- Avoidant (anxious)
- Obsessive-compulsive (anankastic)
- Dependent
- Affective (depressive, hyperthymic, cyclothymic)
Sensitive and suspicious e.g.:
- unreasonable
- Schizoid
- Schizotypal (ICD-10: classified with schizophrenia)
Dramatic and impulsive e.g.:
- Histrionic
- Borderline (emotionally unstable—impulsive)
- self-centered
Antisocial e.g.:
- Antisocial (dissocial)
1.Anxious, Moody and Prone to Worry Personalities:
(i) Avoidant (anxious) personality disorder i.e.:
These people are persistently anxious, ill at ease in company, and fearful of disapproval or criticism. They feel inadequate and are timid. They avoid taking new responsibilities at work and avoid new experiences generally. This tendency to avoid is the basis of the DSM term avoidant.
Characteristics of anxious, moody, worry-prone personalities i.e.:
- Persistently anxious
- Worried about day-to-day problems or health
- Inflexible, obstinate, indecisive (obsessional traits)
- Persistently gloomy and pessimistic or
- Unstable moods, mild elation, or overconfidence alternates with mild depression and/or selfdeprecation
(ii) Obsessive-compulsive (anankastic) personality disorder:
These people are inflexible, obstinate, and rigid in their opinions, and they focus on unimportant detail. They are indecisive, and having made a decision they worry about its consequences.
They are humourless and judgemental, while worrying about the opinions of others. Perfectionism, rigidity, and indecisiveness can make employment impossible.
They appear outwardly controlled but may well be irritated by those who disturb their carefully ordered routine, and may have violent feelings of anger.
(iii) Dependent personality disorder:
These people are passive and unduly compliant with the wishes of others. They lack vigour and self-reliance, and they avoid responsibility. Some achieve their aims by persuading other people to assist them, while protesting their own helplessness.
Some are supported by a more self- reliant partner; left to themselves, they have difficulty in dealing with the demands and also responsibilities of everyday life.
(iv) Persistent mood disorders:
These disorders represent a lifelong tendency to persistent gloom, elation, or varied mood which is abnormal, but not severe enough at any one time to constitute depressive or wild episodes.
Because of the close epidemiological links that we now know exist between these disorders and the mood (affective) disorders, the ‘affective personality disorders’ are now classified among the mood disorders in both DSM-IV and ICD-10. These people have lifelong abnormalities of mood regulation, as follows:
a.Dysthymia (ICD-10 and DSM-IV): Formerly depressive personality disorder. The person is persistently gloomy and pessimistic with little capacity for enjoyment.
b.Cyclothymia (ICD-10 and DSM-IV): Formerly cyclothymic personality disorder. The person’s mood alternates between gloomy and elated over periods of days to weeks. This instability can be particularly disruptive to work and social relationships.
2.Personalities lacking Self esteem and Confidence:
This group is common and important in primary care and general medical practice. These personality features are associate with recurrent depressive moods, eating disorders, and self-harm and are often see among young people who seek help for these problems.
Unfortunately, this group does not appear as a separate entity in the specialist classifications of personality disorder.
Characteristics of personalities lacking self-esteem:
- Lack confidence
- Feel inferior
- Expect criticism
- Strive to please others
- Shyness and social withdrawal/inappropriate efforts to please others
3.Sensitive and Suspicious Personalities:
People in this group are difficult to engage in treatment and they may distrust their doctors:
Characteristics of sensitive and suspicious personalities:
- Sensitive, touchy, irritable; see rebuffs where none exist
- Suspicious, mistrustful
- Cold, detached,show little concern for others,reject help when it is offered
- Eccentric, with unusual ideas about topics such as telepathy
- Self-sufficient
- Lacking concern
(i) Paranoids personality disorder:
These individuals are sensitive and suspicious; they mistrust others and suspect their motives, and are prone to jealousy. They are touchy, irritable, argumentative, and stubborn.
Some of these people have a strong sense of self-importance and special ability, although they may feel that their potential has been stymied by others letting them down or deceiving them.
(ii) Schizoid personality disorder:
These individuals are emotionally cold, self-sufficient, and detached. They are introspective and may have a complex fantasy life.
They show little concern for the opinions of others, and pursue a solitary course through life. When this personality disorder is extreme, the person is cold, callous, and insensitive.
(iii) Schizotypal personality disorder:
These individuals are eccentric and have unusual ideas (e.g. about telepathy and clairvoyance) or ideas of reference. Their speech is abstract and vague, and their affect may be inappropriate to the circumstances. In ICD-10
4.Dramatic and Impulsive Personalities:
characteristics of dramatic and impulsive personalities:
- Seek the limelight, dramatize their problems
- Vain, self-centered
- Demanding of others, to an unreasonable extent, perhaps using ‘emotional blackmail’
- Act a part, self-deceiving, lack awareness of their image to others
- Impulsive, sometimes with harmful behaviours
- Short-lived enthusiasms but lack persistence
- Unrestrained emotional display
(i) Borderline personality disorder:
People with borderline personality represent an important clinical group that presents frequently to healthcare, including A&E departments.
The term ‘borderline’ refers to a combination of features seen also in histrionic and antisocial personalities, which are centred around impulsivity and poor self-control.
The term originates in the now abandoned idea that the condition was related to (on the borderline with) schizophrenia.
Note that ICD-10 uses the term emotionally unstable personality disorder for the same patient group. People with borderline personality disorder have intense but unstable relationships.
They have persistent feelings of boredom and emptiness, with uncertainty about personal identity and a fear of abandonment. Their moods may be unstable, with unwarranted outbursts of anger, and low tolerance of stress.
They are impulsive, and may engage in self damaging behaviours, such as reckless spending or gambling, reckless sex, chaotic eating, and substance abuse. Threats or acts of self-harm may be recurrent.
(ii) Histrionic personality disorder:
These people appear sociable, outgoing, and entertaining but at the same time they are self-centred, prone to short lived enthusiasms, and lack persistence.
Extreme displays of emotion may leave others exhausted while the person recovers quickly and without remorse. Sexually provocative behaviour is common but tender feelings are lacking.
There may be astonishing capacity for self-deception and an ability to persist with elaborate lies long after others have seen the truth.
(iii) self-centered personality disorder:
This disorder is not included in ICD-10. Narcissism is morbid self-admiration. self-centered people have a grandiose sense of self-importance and are preoccupied with fantasies of success, power, and intellectual brilliance.
They crave attention, exploit others, and seek favours but do not return them.
5.Antisocial Personality:
This group corresponds to the dissocial (ICD-10) or antisocial (DSM-IV) groups in the specialist classifications. The difficulties are often increased by abuse of alcohol or illicit drugs.
Characteristics of antisocial personalities:
- Impulsive behaviour, low tolerance of frustration, and lack of consistent striving towards goals, leading to, for example, an unstable work record
- Callous acts, inflicting pain, cruelty, or degradation on others
- Tendency to violence
- Lack of guilt
- Failure to learn from experience, leading to behaviours that persist or escalate despite negative social consequences and legal penalties
- Failure to sustain close relationships, including intimate relationships
- Disregard of the feelings of others
- Family problems, including violence towards partner, and neglect of or violence towards children; frequent separation and divorce
- Often lengthy forensic history, perhaps starting with petty delinquent acts but escalating to callous, violent crime.
Personality Change
By definition, personality is enduring and stable. Small changes often take place very gradually over many years; for example, a person may become less impulsive and aggressive in middle or late life, or a person who is socially anxious and lacking in confidence in their 20s becomes socially and occupationally adept in their 30s and 40s.
The term personality change does not refer to these gradual modifications but to the more abrupt, step-like changes that result sometimes from:
- Injury to, or organic disease of, the brain;
- Residual effects of severe mental disorder, usually schizophrenia;
- Exceptionally severe stressful experiences such as those experienced by hostages or victims of severe torture.
Assessment of Personality
Sources of information:
In everyday life we learn about the personalities of people we know by observing how they respond in various circumstances over the time that we have known them. There are four sources of information:
- A description by someone who knows the patient well, a corroborant. If that person is observant and reliable, this is usually the best source.
- The patient’s own account of their past behaviour in a variety of circumstances. It is less objective but potentially more complete.
- A patient’s own account of their personality. This is also subjective and sometimes influenced by the wish to create a good impression, or by depression or elation.
- The patient’s behaviour in the interview. It is often unreliable because it reflects their current mood and the context of the interview.
The evaluation of personality formed from the last two of these items should be checked by comparing it with an objective record of past achievements and difficulties and, whenever possible, with the accounts of people who know the patient well.
A scheme for assessing personality:
1.Relationships:
This section is concerned with (i) relationships at work (with colleagues, people in authority, and juniors), (ii) relationships with friends, and (iii) intimate relationships.
The interviewer asks whether the patient makes friends easily, has few friends or many, has close friends in whom they can confide, and has lasting friendships. The interviewer also asks whether the patient is sociable and confident in company, or shy and reserved.
Finally, ask about the nature of romantic relationships—their nature, quality, and sense of permanence or instability.
2.Usual mood:
The aim is to discover the person’s usual or habitual mood, not the present or recent mood. There are three elements.
(i) the general character of the person’s mood; is it generally cheerful, middle of the road, or gloomy?
(ii) whether it is stable, changeable, or volatile. If mood is changeable, the interviewer asks how long the changes last, and whether they occur spontaneously or in relation to events.
(iii) whether the person shows his feelings or hides them.
Other traits:
When enquirer about other traits it can help to keep in mind the list which is given below; Each characteristic has a positive as well as a negative side and it is appropriate to ask patients where they lie between the extremes;
Common personality traits (for brevity, only negative attributes are listed; corresponding positive features should also be noted):
- Prone to worry ● Impulsive
- Strict, fussy, rigid ● Attention seeking
- Lacking self-confidence ● Dependent
- Sensitive ● Aggressive
- Suspicious, jealous ● Irritable, quarrelsome
- Untrusting, resentful ● Lacking concern for others
It is useful to check answers by asking for examples from the patient’s recent life, and checking with a corroborant.
Characteristics such as jealousy or lack of feeling for others may not be revealed because the person is ashamed of them or does not recognize their presence.
Observations should be recorded objectively, avoiding value judgements. General terms such as ‘immature’ or ‘inadequate’ should not be used; instead, the interviewer should record in what ways the person has difficulty in meeting the demands of adult life.
4.Attitudes, beliefs, and standards:
Relevant points include attitudes to illness, religious beliefs, and personal standards. Usually, these become apparent when the personal history is being taken, but they can be explored further at this point in the interview.
Usual habits:
Although not strictly part of personality, the person’s usual lifestyle is often relevant. What was their typical daily routine (timeline, structure, activities), and what was their typical daily use of tobacco, alcohol, and illicit drugs?
These aspects of a person’s life may help by (i) indicating possible aetiological factors in current mental illness, or (ii) indicating possible features of current mental illness.
For example, a person whose usual alcohol habit was to drink half a bottle of wine on a Friday and Saturday evening with friends may start to drink more than half a bottle each evening on their own, as ‘self-medication’ to cope with their low mood.
Clinical Features
Tab Content
Sign & Symptoms
Tab Content
Clinical Examination
Tab Content
Diagnosis
If your doctor suspects you have a personality disorder, a diagnosis may be determined by:
- Physical exam. The doctor may do a physical exam and ask in-depth questions about your health. In some cases, your symptoms may link to an underlying physical health problem. Your evaluation may include lab tests and a screening test for alcohol also drugs.
- Psychiatric evaluation. This includes a discussion about your thoughts, feelings and behavior and may include a questionnaire to help pinpoint a diagnosis. Additionally, With your permission, information from family members or others may be helpful.
- Diagnostic criteria in the DSM-5. Your doctor may compare your symptoms to the criteria in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published by the American Psychiatric Association.
Diagnostic criteria:
Each personality disorder has its own set of diagnostic criteria.
However, according to the DSM-5, generally the diagnosis of a personality disorder includes long-term marked deviation from cultural expectations that leads to significant distress or impairment in at least two of these areas:
- The way you perceive and interpret yourself, other people and events
- The appropriateness of your emotional responses
- How well you function when dealing with other people and in relationships
- Whether you can control your impulses
Furthermore, sometimes it can be difficult to determine the type of personality disorder, as some personality disorders share similar symptoms and more than one type may present.
Differential Diagnosis
Complications
Complications are what happen after you have a disease. They are the negative consequences of the disease process.
Investigations
Tab Content
Treatment
Aims of management
Identify and treat any co-morbid psychiatric disorders.
For example: Depression should consider whenever the personality problems have increased recently without another obvious cause, even when the patient does not complain spontaneously of depression.
Treat any associated substance misuse.
Alcohol or other substances may use by people with personality disorder to relieve tension, unhappiness, or feelings of inadequacy. However, they can exacerbate mood disturbance, and their disinhibiting effects can encourage histrionic or aggressive behaviour and self-harm.
Help the patient to deal with or avoid situations that provoke problem behaviours.
for problem behaviours by asking the patient to keep a daily diary of the behaviours and the situations in which they occur. For example, aggression may be provoked by social rejection, which is the response of others to the patient’s lack of social skills. Treatment would then include social skills training.
Provide general support to reduce tension and increase self-esteem.
particularly the effects on any children living with the patient. Although these enquiries are particularly important when the person is aggressive, the problems of people who are persistently anxious, histrionic, or suspicious may also affect their families.
Support and help the family.
This may be needed especially when the personality disorder is of the aggressive or antisocial kind. If a mother has a personality disorder, the health and development of the children should assesse, and appropriate steps taken to alleviate any problems.
Psychotherapy:
During psychotherapy with a mental health professional, you can learn about your condition and talk about your moods, feelings, thoughts and behaviors. You can learn to cope with stress and manage your disorder.
First of all, Psychotherapy may be provided in individual sessions, group therapy, or sessions that include family or even friends. There are several types of psychotherapy — your mental health professional can determine which one is best for you.
You may also receive social skills training. During this training you can use the insight and knowledge you gain to learn healthy ways to manage your symptoms and reduce behaviors that interfere with your functioning and relationships.
Family therapy provides support and education to families dealing with a family member who has a personality disorder.
Medications:
There are no medications specifically approved by the Food and Drug Administration (FDA) to treat personality disorders. However, several types of psychiatric medications may help with various personality disorder symptoms.
- Antidepressants. Antidepressants such as the SSRI fluoxetine, may be useful if you have a depressed mood, anger, impulsivity, irritability or hopelessness, which may be associated with borderline personality disorders.
- Mood stabilizers. Such as lithium carbonate and other anticonvulsants are useful. Additionally, As their name suggests, mood stabilizers can help even out either mood swings or reduce irritability, impulsivity and aggression.
- Antipsychotic medications. Also called neuroleptics, these may be helpful if your symptoms include losing touch with reality (psychosis) or in some cases if you have either anxiety or anger problems.
- Anti-anxiety medications. These may help if you have anxiety, agitation or insomnia. But in some cases, they can increase impulsive behavior, so they’re avoided in certain types of personality disorders.
Prevention
Tab Content
Homeopathic Treatment
Useful Remedies:
Calcarea carbonica:
This remedy is usually indicated for dependable solid people who become overwhelmed from physical illness or too much work and start to fear a breakdown.Their thoughts can be muddled and confused when tired, which adds to the anxiety. Worry may agitate them, and a nagging dread of disaster (to themselves or others) may develop. Fear of heights and claustrophobia are also common. A person who needs this remedy is often chilly and sluggish, has a craving for sweets, and is easily fatigued.
Ignatia Amara:
A sensitive person who is anxious because of grief, loss, disappointment, criticism, loneliness (or any stressful emotional experience) may benefit from this remedy. A defensive attitude, frequent sighing, and mood swings are other indications. The person may burst unexpectedly into either tears or laughter. Headaches that feel like a nail driven into the side of the head, and cramping pains in the abdomen or back, are often seen when this remedy is needed.
Naja mentals:
Sense of duality the feeling of being split into two, of having two wills. Conflict between higher (human) and lower (animal) nature, strong sense of duty (which in the duality-neglect), feels as if he is a failure. Delusion he has suffered-broods over imaginary troubles (which in the duality suffering wrong and doing wrong to others). Timidity fear of rain, fear of being abandoned.
Keynotes:
Affinities: Cerebellum, Medulla, Nerves, Heart, respiration- throat. Worse: specifically lying on left side. After sleep, after menses. Air (cold; drafts) Damp Weather. Tight clothing. Alcohol. Exertion. Talking. Walking. Night. Touch. 3 pm. Stimulants. On the other hand, Better: Walking and riding in open air. Sneezing. Lying on right side. Very sensitive to cold- desires warmth. Colds that turn to asthma. Sensation as if organs are drawn together.
Some other remedies, which can be used in these cases are:
apis, hyoscyamus, lachesis, cannabis sativa, spongia, aurum met, derris pin- nata, opium, agaricus, bovista, staphysagria, meliotus, tellurium, gelse- mium, bryonia, etc.
Diet & Regimen
Lifestyle and Home Remedies
Lifestyle and home remedies:
Along with your professional treatment plan, consider these lifestyle and self-care strategies:
Be an active participant in your care.
Generally, This can help your efforts to manage your personality disorder. Don’t skip therapy sessions, even if you don’t feel like going. Think about your goals for treatment and work toward achieving them.
Take your medications as directed.
Even if you’re feeling well, don’t skip your medications. If you stop, symptoms may come back. Additionally, You could also experience withdrawal-like symptoms from stopping a medication too suddenly.
Learn about your condition.
In brief, Education about your condition can empower you and motivate you to stick to your treatment plan.
Get active.
Physical activity can help manage many symptoms, such as depression, stress and anxiety. It can also counteract the effects of some psychiatric medications that may cause weight gain. Consider walking, jogging, swimming, gardening or taking up another form of physical activity that you enjoy.
Avoid drugs and alcohol.
Alcohol also street drugs can worsen personality disorder symptoms or interact with medications.
Get routine medical care.
Don’t neglect checkups or skip visits to your primary care professional, especially if you aren’t feeling well. You may have a new health problem that needs to address, or you may be experiencing side effects of medication.
Caring and support:
Having a personality disorder makes it hard to engage in behavior and activities that may help you feel better. In detail, Ask your doctor or therapist how to improve your coping skills and get the support you need.
Furthermore, If you have a loved one with a personality disorder, work with his or her mental health professional to find out how you can most effectively offer support and encouragement.
You may also benefit from talking with a mental health professional about any distress you experience.
All in all, A mental health professional can also help you develop boundaries and self-care strategies so that you’re able to enjoy and succeed in your own life.
Do’s and Dont’s
Tab Content
Terminology
Tab Content
References
FAQ
Frequently Asked Questions
What is Personality Disorders?
A personality disorder is a type of mental disorder in which you have a rigid and unhealthy pattern of thinking, functioning and behaving.
Homeopathic Medicines used by Homeopathic Doctors in treatment of Personality Disorders?
- Calcarea carbonica
- Ignatia Amara
- Naja
- Apis
- Hyoscyamus
- Lachesis
What causes Personality Disorders?
- Genetic factors
- Childhood experience
- Injury to the brain at birth
- Abnormal brain development
- Serotonin
- Parenting
What are the symptoms of Personality Disorders?
A person may become less impulsive and aggressive in middle or late life, or a person who is socially anxious and lacking in confidence in their 20s becomes socially and occupationally adept in their 30s and 40s.
Give the types of ?
- Anxious, moody, and prone to worry
- Lacking self-esteem and confidence
- Sensitive and suspicious
- Dramatic and impulsive
- Aggressive and antisocial
Also Search As
Frequently Asked Questions (FAQ)
XYZ
XXX
XYZ
XXX
XYZ
XXX
How can I find reputable homeopathy clinics or homeopathic doctors in my area?
You can found Homeopathic Clinic For XXXX by searching for
Specific city Examples are
You can also search for near you Examples are