In mania the life-time risk of unbalanced episode is about 0.81%. Additionally, This disorder tends to occur in episodes lasting usually 3-4 months, followed by complete clinical recovery.
The future episodes can be unbalanced, depressive or mixed.
A unbalanced episode is typically characterized by the following features (which should last for at least one week and cause disruption in occupational and social activities).
● Hypomania:
This term refers to a state in which wild symptoms are present and noticeable, but they do not cause a serious degree of functional impairment.
● Mild mania:
Physical activity and speech are increased, mood is labile, mainly euphoric but at times irritable, ideas are expansive, and the patient often spends more than he can afford. By definition, there is significant social impairment in this and the other patterns of mania.
● Moderate mania:
In brief, there is marked over-activity with pressure also disorganization of speech, the euphoric mood is increasingly interrupted by periods of irritability, hostility, and depression, and grandiose also other preoccupations may become delusional.
● Severe mania:
There is frenzied overactivity, thinking is incoherent and delusions become increasingly bizarre, and hallucinations are experienced. Very rarely, however, the patient becomes immobile and mute instead of overactive and talkative (in other words, wild stupor).
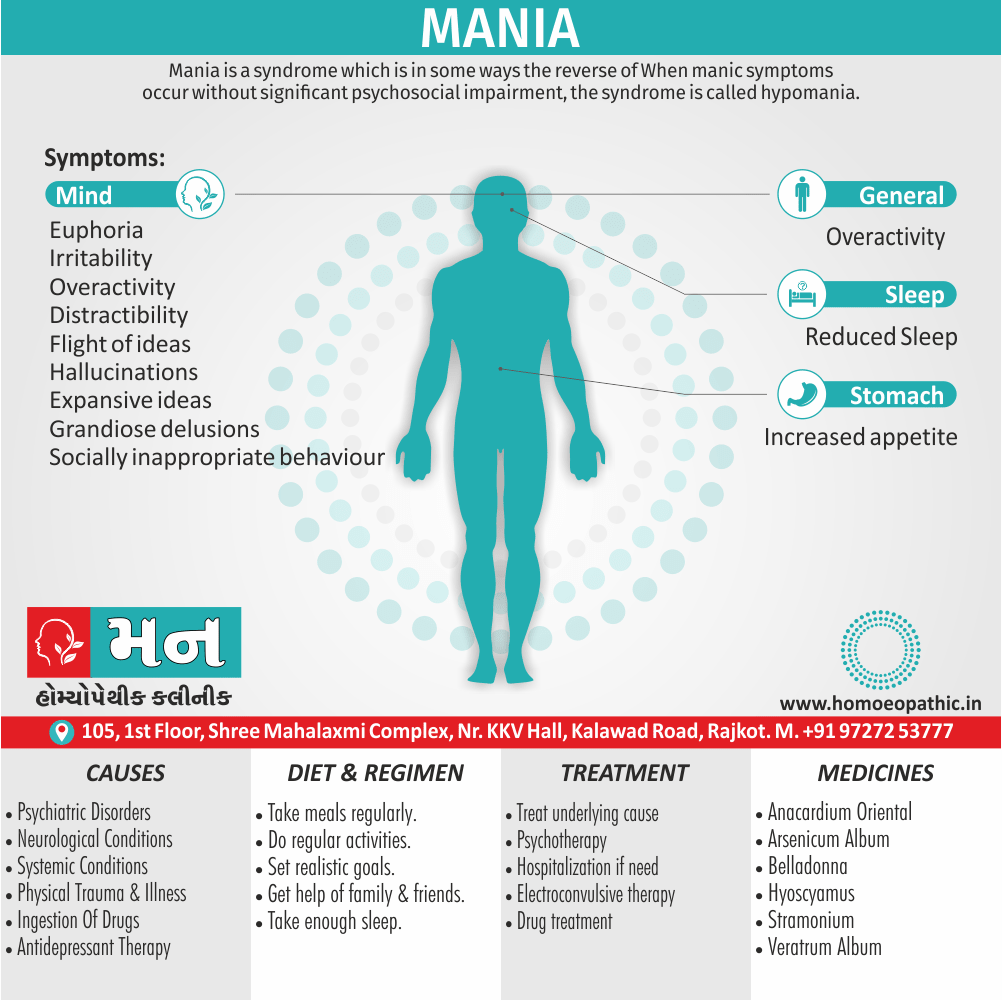
| Mood |
| ● Euphoria |
| ● Irritability |
| Appearance Behaviour |
| ● Overactivity |
| ● Distractibility |
| ● Socially inappropriate behaviour |
| ● Reduced sleep |
| ● Increased appetite |
| ● Increased libido |
| Thinking and speech |
| ● Flight of ideas |
| ● Expansive ideas |
| ● Grandiose delusions |
| ● Hallucinations |
| Impaired insight |
Diagnosis:
DSM-IV diagnostic criteria for mania i.e.:
A. A distinct period of abnormally and persistently elevated, expansive, or irritable mood, lasting at least 1 week (or any duration if hospitalization is necessary).
B. During the period of mood disturbance, three (or more) of the following symptoms have persisted (four if the mood is only irritable) and have been present to a significant degree i.e.:
- Inflated self-esteem or grandiosity
- Decreased need for sleep (e.g. feels rested after only 3 hours of sleep)
- More talkative than usual or pressure to keep talking
- Flight of either ideas or subjective experience that thoughts are racing
- Distractibility (i.e. attention too easily drawn to unimportant or irrelevant external stimuli)
- Increase in goal-directed activity (either socially, at work or school, or sexually) or out of control motor agitation.
C. The symptoms do not meet criteria for a Mixed Episode.
D. A mood disturbance is sufficiently severe to cause marked impairment in occupational functioning or in usual social activities or relationships with others, or to necessitate hospitalization to prevent harm to self or others, or there are psychotic features.
E. The symptoms are not due to the direct physiological effects of a substance (e.g. a drug of abuse, a medication, or other treatment) or a general medical condition (e.g. hyperthyroidism).
Differential diagnosis of unbalanced disorders
- Schizophrenia
- Dementia
- Endocrine disorders such as Hypothyroid
- Abuse of stimulant drugs
General aspects of the treatment of mania:
Milder wild episodes may treat as an outpatient, but more severe disorders with associated loss of judgement will almost always need initial treatment as an inpatient. When the disorder is more severe, compulsory admission is likely to need.
Almost all patients with a wild episode will need drug treatment (Anti-psychotic drugs). The clinical status should monitor frequently.
Progress is judge not only by the mental state and general behavior, but also by the pattern of sleep and by the regaining of any weight lost during the illness. As progress continues, anti-psychotic drug treatment is reduce gradually.
It is important, however, not to discontinue the drug too soon, otherwise relapse may occur. During treatment a careful watch should be kept for the appearance of depressive symptoms because transient but profound depressive mood change and depressive ideas are common among unbalanced patients.
In either case, suicidal ideas may appear. A sustained change to a depressive syndrome may require treatment, including with antidepressant drugs which should use cautiously to avoid precipitation of a unbalanced relapse.
Specific treatments for mania:
Anti-psychotic drugs i.e.:
Anti-psychotic drugs have an established place in the treatment of mania. An atypical anti-psychotic, such as olanzapine, quetiapine, or risperidone, is therefore usually the first-choice treatment.
Antipsychotics should generally not be used to control behavior because the doses required for this effect are high and adverse effects are therefore more likely.
A benzodiazepine such as lorazepam or diazepam should be used instead.
Lithium i.e.:
Lithium is effective in mania, but less so than anti-psychotic drugs, and it can be difficult to use safely in severely disturbed patients.
It is therefore used mainly in patients with milder unbalanced episodes, especially when it is intended to continue the treatment in the long term to prevent relapse.
It is also used in combination with anti-psychotics—caution is required when used in combination with haloperidol because extra-pyramidal effects occur commonly.
Anti-epileptic drugs i.e.:
Valproate is effective in acute mania. It is slightly less effective than anti-psychotics, but causes fewer adverse effects.
Thus, it may be particularly useful in patients who are not currently taking a long-term mood stabilizer, and who have a mild wild illness without psychotic features.
An advantage of valproate over lithium in the acute phase is that a high loading dose can be given, which leads to a more rapid response and shorter hospital stays.
Carbamazepine is another anti-epileptic drug that can be used in mania.
Electroconvulsive therapy i.e.:
Clinical experience indicates that ECT has a powerful therapeutic effect in mania.
Nevertheless, ECT is not a first-line treatment; its use is mainly in the uncommon cases when anti-psychotic drugs are ineffective and the patient is so seriously disturbed that to spend time trying further medication or awaiting natural recovery is not justified.
Homoeopathic Treatment:
Homeopathic Treatment of Mania
Homeopathy treats the person as a whole. It means that homeopathic treatment focuses on the patient as a person, as well as his pathological condition. The homeopathic medicines selected after a full individualizing examination and case-analysis.
Which includes
- The medical history of the patient,
- Physical and mental constitution,
- Family history,
- Presenting symptoms,
- Underlying pathology,
- Possible causative factors etc.
A miasmatic tendency (predisposition/susceptibility) also often taken into account for the treatment of chronic conditions.
What Homoeopathic doctors do?
A homeopathy doctor tries to treat more than just the presenting symptoms. The focus is usually on what caused the disease condition? Why ‘this patient’ is sick ‘this way’?
The disease diagnosis is important but in homeopathy, the cause of disease not just probed to the level of bacteria and viruses. Other factors like mental, emotional and physical stress that could predispose a person to illness also looked for. Now a days, even modern medicine also considers a large number of diseases as psychosomatic. The correct homeopathy remedy tries to correct this disease predisposition.
The focus is not on curing the disease but to cure the person who is sick, to restore the health. If a disease pathology not very advanced, homeopathy remedies do give a hope for cure but even in incurable cases, the quality of life can greatly improve with homeopathic medicines.
Homeopathic Medicines for Mania:
The homeopathic remedies (medicines) given below indicate the therapeutic affinity but this is not a complete and definite guide to the homeopathy treatment of this condition. The symptoms listed against each homeopathic remedy may not be directly related to this disease because in homeopathy general symptoms and constitutional indications also taken into account for selecting a remedy, potency and repetition of dose by Homeopathic doctor.
So, here we describe homeopathic medicine only for reference and education purpose. Do not take medicines without consulting registered homeopathic doctor (BHMS or M.D. Homeopath)
Medicines:
Lillium Tigrinum
- Lillium Tigrinum is of great help in treating increased energy levels in Bipolar Disorder where the main symptom is extreme restlessness and difficulty in sitting still at one place.
- Another feature to look out for while choosing Lillium Tigrinum is when a patient shows great hurriedness without any ambition or aim.
- The patient requiring this medicine usually has a heart or uterine disease associated with the mental symptoms.
Cannabis Indica
- Cannabis Indica is another helpful remedy for treating increased energy levels in Bipolar Disorder.
- One noticeable symptom for which this medicine is of great help is when the patient has bouts of uncontrollable laughter on listening to every little word spoken, which may not even be funny, and excessive talkativeness.
- The patient requiring Cannabis Indica is full of thoughts crowding the brain at one time, making the patient forgetful of words while talking.
Belladonna
- Belladonna works very well for those patients of Bipolar Disorder who show marked violent behavior and violence occurs in fits that come and go suddenly and the patient even bites and strikes the person near him or her.
- Another symptom of violence where Belladonna is beneficial as a cure is when the patient spits on people and the face turns red.
Ignatia Amara
- In general, Ignatia Amara is one of the best remedies for treating sadness experienced by a patient in the depressive phase of Bipolar Disorder.
- Moreover, The patients requiring this medicine usually have a history of long-held grief like the death of a family member or close friend or in cases where the disease has originated after disappointed love affections or from suppressed emotions.
- Ignatia Amara is a very helpful remedy for patients who sit silently also weep or brood over the past.
Sepia
- Sepia is also beneficial for treating sadness during the depression stage of Bipolar Disorder.
- The main symptoms for using this medicine are constant weeping, indifferent behavior towards people and even family members who were once much respected and loved, and lack of interest in doing any mental or physical work.
Aurum Metallicum
- Aurum Metallicum is an excellent medicine for treating those cases of depression in Bipolar Disorder where suicidal thoughts predominate and the patient feels hopeless and worthless and has persistent suicidal thoughts.
Natrum Sulphuricum
- Natrum Sulphuricum is another remedy of great help for a patient in whom suicidal thoughts are marked and they has to apply much self-control to stop themselves from actually died by suicide.
- Another symptom that calls for the use of medicine Natrum Sulphuricum is gloominess.
- When the patient of Bipolar Disorder feels sad even when listening to lively music and has an aversion to talk or be spoken to, Natrum Sulphuricum is very beneficial.
Frequently Asked Questions
What is Mania?
Mania is a syndrome which is in some ways the reverse of depression. When excited symptoms occur without significant psychosocial impairment, the syndrome is called hypomania.
Homeopathic Medicines used by Homeopathic Doctors in treatment of Mania?
- Lillium Tigrinum
- Cannabis Indica
- Belladonna
- Ignatia Amara
- Sepia
- Aurum Metallicum
- Natrum Sulphuricum
What causes Mania?
- Hypomania
- Mild mania
- Moderate mania
- Severe mania
What are the symptoms of Mania?
- Euphoria
- Irritability
- Overactivity
- Distractibility
- Socially inappropriate behaviour
- Reduced sleep
- Increased appetite
- Increased libido
Psychiatry, Fourth Edition – Oxford Medical Publications -SRG-by John Geddes, Jonathan Price, Rebecca McKnight