[vc_row][vc_column][vc_column_text]
Learning Disabilities:
Definition:
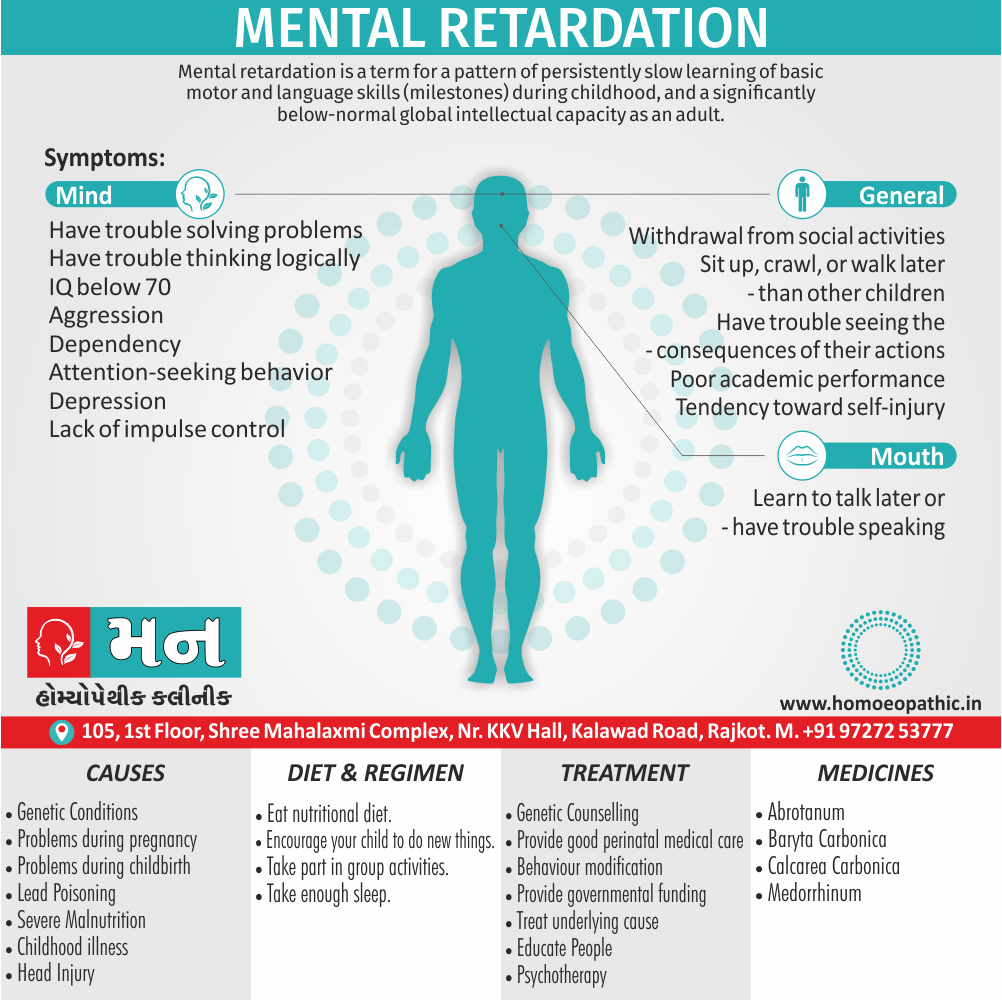
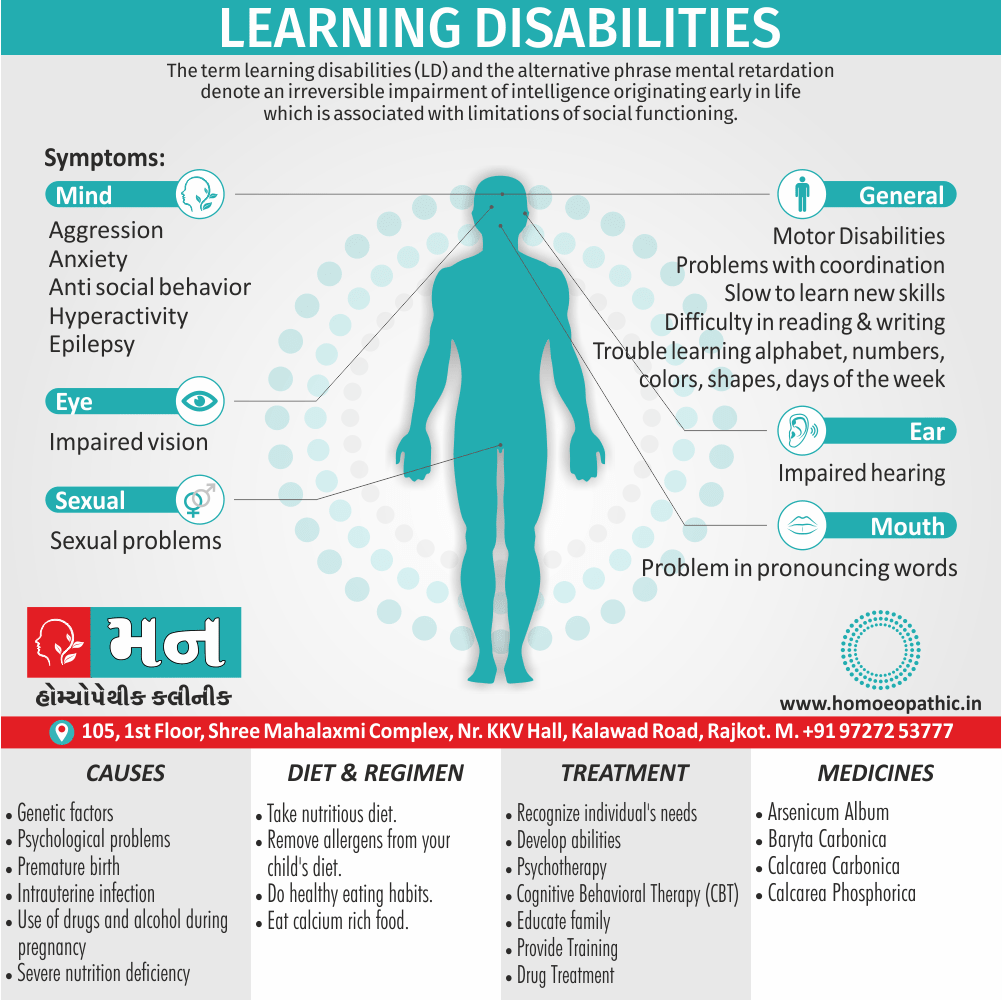
The term learning disabilities (LD) and the alternative phrase mental retardation denote an irreversible impairment of intelligence originating early in life which is associated with limitations of social functioning. [2]
Moreover, The word “disability” draws attention to what the DSM definition refers to as ‘concurrent deficits also impairments in adaptive behaviour, taking into account the person’s age’. [2]
What are learning disabilities?
Kids with learning disabilities aren’t either lazy or foolish. In fact, most are just as smart as everyone else. Additionally, Their brains are simply wired differently. This difference affects how they receive and process information.
Simply put, children and adults with learning disabilities see, hear, and understand things differently. In detail, This can lead to trouble with learning new information and skills also putting them to use. All in all, The most common types of learning disabilities involve problems with reading, writing, math, reasoning, listening, and speaking. [1][/vc_column_text][/vc_column][/vc_row][vc_row][vc_column][vc_tta_tour color=”turquoise” active_section=”1″][vc_tta_section title=”Overview” tab_id=”1548500019927-ccbf15a5-1f58″][vc_column_text]
Learning Disabilities:
Does your child struggle with school? Does they dread reading out loud, writing an essay, or tackling a math problem? While every kid has trouble with homework from time to time, if a certain area of learning is consistently problematic, it might indicate a learning disorder.
By understanding all you can about learning disabilities, you can ensure your child gets the right help to overcome classroom challenges also succeed in life. [1]
Besides this, LD is not a clinical diagnosis in its own right, just a way of describing a particular clinical syndrome of impairments with disability and handicaps.
The terms impairment, disability, and disability are not interchangeable. Lastly, The value of their use is in describing an individual’s specific needs, irrespective of their etiological diagnosis. [2]
Impairment i.e.
It is any loss or abnormality of psychological, physical, or anatomical structure or function. It is not dependent upon etiology. [2]
Disability i.e.
It is any restriction in the ability to perform an activity within the range considered normal for a human at a corresponding level of development. [2]
A disability i.e.
It is a disadvantage for a person, due to their impairment or disability, that prevents them from fulfilling a role that is normal for that individual. [2]
[/vc_column_text][/vc_tta_section][vc_tta_section title=”Epidemiology” tab_id=”1548500020010-babb8abe-36b7″][vc_column_text]The definition of LD as an IQ < 70 is based upon the assumption that IQ is normally distributed with a mean of 100 and standard deviation of 15.
Two standard deviations below the mean is 70, representing 2.5 percent of the population. However, reported rates of LD are actually 2–3 per cent. This is because average IQ varies with a number of factors i.e.:
- Country: Learning disabilities are more common in developing than developed countries. This is primarily due to preventable causes (e.g. iodine deficiency).
- Genetics: Different ethnic groups show variable intellectual abilities.
- Age: Prevalence of LD is higher in child than adult cohorts, with a peak at 10 years. This is partly due to the reduced life expectancy of some individuals with LD, but also due to diagnostic bias.
Not all individuals with an IQ < 70 have LD; they must also have impairment of functioning. [2][/vc_column_text][/vc_tta_section][vc_tta_section title=”Sign & Symptoms” tab_id=”1548501117566-3341bb5c-24e9″][vc_column_text]
Learning disabilities look very different from one child to another. One child may struggle with reading and spelling, while another loves books but can’t understand math.
Still another child may have difficulty understanding what others are saying or communicating out loud. The problems are very different, but they are all learning disorders. [1]
Signs and symptoms of learning disabilities: Preschool age:
- Problems pronouncing words
- Trouble finding the right word
- Difficulty rhyming Trouble learning the alphabet, numbers, colors, shapes, days of the week
- Difficulty following directions or learning routines
- Difficulty controlling crayons, pencils, also scissors, or coloring within the lines
- Trouble with buttons, zippers, snaps, learning to tie shoes
Symptoms and signs of learning disabilities: Ages 5-9:
- Trouble learning the connection between letters also sounds
- Unable to blend sounds to make words
- Confuses basic words when reading
- Slow to learn new skills
- Consistently misspells words also makes frequent errors
- Trouble learning basic math concepts
- Difficulty telling time also remembering sequences
Signs and symptoms of learning disabilities: Ages 10-13:
- Difficulty with reading either comprehension or math skills
- Trouble with open-ended test questions and word problems
- Dislikes reading and writing; avoids reading aloud Poor handwriting
- Poor organizational skills (for example; bedroom, homework, desk is messy also disorganized)
- Trouble following classroom discussions also expressing thoughts aloud
- Spells the same word differently in a single document [1]
[/vc_column_text][/vc_tta_section][vc_tta_section title=”Causes” tab_id=”1548501115796-781b1021-3ffe”][vc_column_text]Factors that might influence the development of learning disorders include:
Family history and genetics:
- In brief, A family history of learning disorders increases the risk of a child developing a disorder.
Prenatal and neonatal risks:
- Poor growth in the uterus (severe intrauterine growth restriction), exposure to alcohol or drugs before being born, premature birth, also very low birthweight have been linked with learning disorders.
Psychological trauma:
- Either, Psychological trauma or abuse in early childhood may affect brain development and increase the risk of learning disorders.
Physical trauma:
- Head injuries or nervous system infections might play a role in the development of learning disorders.
Environmental exposure:
Exposure to high levels of toxins, such as lead, has been linked to an increased risk of learning disorders.[/vc_column_text][/vc_tta_section][vc_tta_section title=”General Types” tab_id=”1548501238429-261a8287-a459″][vc_column_text]
Paying attention to developmental milestones can help you identify learning disorders:
Problems with reading, writing, and math i.e.:
Learning disabilities are often grouped by school-area skill set. If your child is in school, the types of learning disorders that are most conspicuous usually revolve around reading, writing, or math. [1]
Learning disabilities in reading (dyslexia) i.e.:
There are two types of learning disabilities in reading. Basic reading problems occur when there is difficulty understanding the relationship between sounds, letters and words. Reading comprehension problems occur when there is an inability to grasp the meaning of words, phrases, and paragraphs. [1]
Signs of reading difficulty include problems with:
- letter and word recognition
- understanding words and ideas
- reading speed and fluency
- general vocabulary skills
Learning disabilities in math (dyscalculia) i.e.:
Learning disabilities in math vary greatly depending on the child’s other strengths and weaknesses. A child’s ability to do math will be affected differently by a language learning disability, or a visual disorder or a difficulty with sequencing, memory or organization.
A child with a math-based learning disorder may struggle with memorization and organization of numbers, operation signs, and number “facts” (like 5+5=10 or 5×5=25). Children with math learning disorders might also have trouble with counting principles (such as counting by twos or counting by fives) or have difficulty telling time. [1]
Learning disabilities in writing (dysgraphia) i.e.:
Learning disabilities in writing can involve the physical act of writing or the mental activity of comprehending and synthesizing information.
Basic writing disorder refers to physical difficulty forming words and letters. Expressive writing disability indicates a struggle to organize thoughts on paper.
Symptoms of a written language learning disability revolve around the act of writing. They include problems with:
- neatness and consistency of writing
- accurately copying letters and words
- spelling consistency
- writing organization and coherence [1]
Other types of learning disabilities and disorders i.e.:
Reading, writing, and math aren’t the only skills impacted by learning disorders. Other types of learning disabilities involve difficulties with motor skills (movement and coordination), understanding spoken language, distinguishing between sounds, and interpreting visual information. [1]
Learning disabilities in motor skills (dyspraxia) i.e.:
Motor difficulty refers to problems with movement and coordination whether it is with fine motor skills (cutting, writing) or gross motor skills (running, jumping).
A motor disability is sometimes referred to as an “output” activity meaning that it relates to the output of information from the brain. In order to run, jump, write or cut something, the brain must be able to communicate with the necessary limbs to complete the action.
Signs that your child might have a motor coordination disability include problems with physical abilities that require hand-eye coordination, like holding a pencil or buttoning a shirt. [1]
Learning disabilities in language (aphasia/dysphasia) i.e.:
Language and communication learning disabilities involve the ability to understand or produce spoken language. Language is also considered an output activity because it requires organizing thoughts in the brain and calling upon the right words to verbally explain something or communicate with someone else.
Signs of a language-based learning disorder involve problems with verbal language skills, such as the ability to retell a story and the fluency of speech, as well as the ability to understand the meaning of words, parts of speech, directions, etc. [1]
Auditory and visual processing problems i.e.:
Auditory processing disorder
Professionals may refer to the ability to hear well as “auditory processing skills” or “receptive language.” The ability to hear things correctly greatly impacts the ability to read, write and spell.
An inability to distinguish subtle differences in sound, or hearing sounds at the wrong speed make it difficult to sound out words and understand the basic concepts of reading and writing. [1]
Visual processing disorder
Problems in visual perception include missing subtle differences in shapes, reversing letters or numbers, skipping words, skipping lines, misperceiving depth or distance, or having problems with eye–hand coordination.
Professionals may refer to the work of the eyes as “visual processing.” Visual perception can affect gross and fine motor skills, reading comprehension, and math. [1]
Common types of learning disabilities:
Dyslexia – Difficulty with reading
Problems reading, writing, spelling, speaking
Dyscalculia – Difficulty with math
Problems doing math problems, understanding time, using money
Dysgraphia – Difficulty with writing Problems with handwriting, spelling, organizing ideas
Dyspraxia (in other words; Sensory Integration Disorder) – Difficulty with fine motor skills Problems with hand-eye coordination, balance, manual dexterity
Dysphasia/Aphasia – Difficulty with language
Problems understanding spoken language, poor reading comprehension
Auditory Processing Disorder – Difficulty hearing differences between sounds Problems with reading, comprehension, language
Visual Processing Disorder – Difficulty interpreting visual information Problems with reading, math, maps, charts, symbols, pictures [1]
[/vc_column_text][/vc_tta_section][vc_tta_section title=”General problems” tab_id=”1548501239881-0feaaa83-a6b3″][vc_column_text]
It can be divided into 4 categories i.e.: [2]
- Firstly, Emotional and behavioural problems
- Secondly, Physical disorders among people with learning disability
- Thirdly, Effects of learning disability on the family
- Fourthly, Specific psychiatric disorders
1. Emotional and behavioural problems:
Behavioural disorders, at any given age, are more common in individuals with learning disabilities than in the general population. There are a variety of common behaviours which can be difficult to manage.
- Aggression and/or antisocial behaviour: this may be shouting and screaming, faecal smearing, and selfinduced vomiting in youngsters.
- Self-injury: For instance; biting, cutting, burning, and head banging. These are inversely proportionate to IQ in frequency. Overall, 40 per cent of children also 20 per cent of adults with LD self-injure.
- Stereotyped behaviours such as rocking, mannerisms, and flapping usually seen in autistic spectrum disorders. The presence of these does not necessarily mean the child is autistic.
- Hyperactivity
- Anxiety
- Social withdrawal
- Sexual problems: Some people with LD show a child-like curiosity about other people’s bodies, which can be misunderstood as sexual. Many need sympathetic help in understanding sexual feelings at and after puberty.
Behavioural problems are usually multifactorial in origin, combining genetics, characteristics inherent to the specific cause of the LD, and environmental factors.
Causes of behavioural problems in learning disability i.e.: [2]
Table no.19.5 page no.194 (1.4)
2. Physical disorders among people with learning disability:
Physical disorders are most frequent among those with severe and profound LD, many of whom have motor disabilities (20–30 per cent) or epilepsy (40 per cent).
- Impaired hearing or vision may add an important additional obstacle to normal cognitive development, and is found in 10–20 per cent of those with an IQ < 35.
- Motor disabilities, which are frequent, include spasticity, ataxia, and athetosis, and are often due to cerebral palsy.
- Epilepsy is frequent in LD and may present at any age. It needs to be carefully distinguished from stereotypies or mannerisms (e.g. rolling eyes) and from episodes of complete social withdrawal. All forms of epilepsy may occur, and the seizure pattern may change over time. Increased frequency of seizures may indicate physical illness, stress, or non-epileptic seizures. Severe epilepsy can cause permanent loss of intellectual ability in anyone, and this is more frequent in those with LD to begin with. Epilepsy can usually be controlled effectively with antiepileptic drugs.[2]
3. Effects of learning disability on the family:
- Prenatal diagnosis: now means that parents can be put in a situation of having to make choices about an unborn child. This is extremely stressful, and the couple will need advice and counselling from professionals to make the choice that is best for them.
- Rejection: When a newborn child is found to have LD, the parents are distressed and some reject the child at first, although this rejection seldom lasts long. More often the diagnosis is not made until after the first year of life. When this happeens many experience a period of depression, guilt, shame, or anger. If the child also has a physical disability, these problems are greater.
- Depression and social problems: It is very common, especially amongst those parents who cannot work or socialize due to having to care for their child. Siblings may also be affected, either by the stress and anxiety caused by family life, or from reduced parental attention. For these reasons, the whole family of a child with learning disability needs long term support.
- Specific problems may arise when the parents of a severely LD child become too old or unwell to take care of their dependent child.[2]
4. Specific psychiatric disorders:
-
Attention deficit hyperactivity disorder (ADHD) i.e.:
ADHD is seen in up to 20 per cent of children with LD. Attention and concentration should be judged against those of a child of a comparable developmental, not chronological, age. Hyperactivity is typically the most prominent symptom, and usually responds well to stimulants.
-
Autistic spectrum disorders (ASD) i.e.:
ASD are more common in people with LD than in the rest of the population, with a prevalence of about 1–2 per cent in all children with LD, and about 5 per cent in people with severe LD. There is a particular association with tuberous sclerosis, congenital rubella, severe epilepsy, and phenylketonuria. Most children with LD will try to communicate, use gestures/facial expressions, and display emotions, whilst these are reduced or absent in ASD.
When people with LD develop a depressive disorder they are less likely than people of normal intelligence to complain of low mood or to express depressive ideas. Diagnosis has to be made mainly on observable features such as an appearance of sadness, reduction of appetite, disturbance of sleep, retardation, or agitation.
Atypical features such as a regression to child-like behaviours, incontinence, and loss of social skills are more common. A severely depressed patient with adequate verbal abilities may describe depressive ideas, delusions, or hallucinations. A few of these patients make attempts at suicide, although these are usually poorly planned.
Classical bipolar disorder I is occasionally seen in LD, with rapid cycling being a prominent feature.
Mania has to be diagnosed mainly on overactivity and behavioural signs indicating excitement and irritability.
-
Anxiety disorders i.e.:
The most commonly reported anxiety disorders are simple phobia, social phobia, and generalized anxiety disorder (GAD). Behaviour problems, irritability, withdrawal, insomnia, and somatic complaints are the usual symptoms seen.
Anxiety disorders occasionally improve with stress reduction strategies, but are much harder to treat than in the general population.Similarly, stress-related and adjustment disorders occur commonly among people with mild and moderate LD.
-
Psychosis i.e.:
In individuals with mild LD, the classical symptoms of schizophrenia (or other psychoses) are present, and diagnosis is relatively simple.
Delusions frequently contain ideas gathered from the person’s immediate environment, for example television shows.
Catatonic symptoms are much more common. The negative symptoms of schizophrenia appear early, and are relatively treatment resistant. When the IQ is below 45, it is difficult to make a definite diagnosis of schizophrenia.
-
Delirium and dementia i.e.:
Delirium is lower in those with LD. Disturbed behaviour resulting from delirium may be the first indication of physical illness.
Dementia causes a progressive global decline in intellectual and social functioning from the previous level. It presents at a younger age, and may progress more quickly, in those with severe or profound LD. Nocturnal confusion (‘sun downing’), forgetting the usual domestic routine, and late-onset epilepsy are sensitive markers of dementia.
-
Personality disorder i.e.:
Epidemiological data suggests that personality disorders are common amongst people with mild LD and sometimes lead to greater problems in management than the learning problems. Because psychological development is delayed, the diagnosis is not generally made until the age of 20 years. [2][/vc_column_text][/vc_tta_section][vc_tta_section title=”Diagnosis” tab_id=”1548501375985-ed2043f5-a310″][vc_column_text]
Diagnosis of psychiatric disorder in learning disability:
All types of mental disorder may occur at any degree of LD, but at the severe level the most frequent are autism, hyperkinetic syndrome, stereotyped movements, pica, and self-mutilation. Those patients with epilepsy have a higher risk of serious psychiatric disorders.
The assessment and management of all psychiatric diagnoses are as for any patient presenting with the corresponding symptoms.[2]
Diagnosing a learning disability is a process. It involves testing, history taking, and observation by a trained specialist.
- Clinical psychologists
- School psychologists
- Child psychiatrists
- Educational psychologists
- Developmental psychologists
- Neuropsychologist
- Psychometrist
- Occupational therapist (tests sensory disorders that can lead to learning problems)
- Speech and language therapist [1]
-
Diagnosis:
1.Patients may have insufficient verbal ability to describe abnormal experiences accurately (the level of ability corresponds to an IQ level of about 50).
2. Some people with LD are suggestible and may answer positively to a question about a symptom when they have not in fact experienced it.
For the above reasons, diagnosis often has to be based on reports by others of changes in the patient’s behaviour.
3. Some causes of LD also cause abnormal behaviour. Behaviour problems due to psychiatric disorder may be wrongly ascribed to this other cause, or vice versa.
4. LD is associated with autism, and some of the symptoms of autism can be mistaken for those of another psychiatric disorder, for example obsessive-compulsive disorder.
5. Physical illness or stressful events can cause changes in behaviour, and both should be considered before the diagnosis of mental disorder made.[2]
-
Physical examination:
The physical examination is best carried out by a paediatrician with knowledge of developmental and neurological disorders. It should include the recording of head circumference, height, and weight. Look carefully for dysmorphic features and congenital abnormalities.
It may be helpful to examine close relatives to determine if any abnormalities are present in them too.
A full neurological examination is essential, including speech and language, hearing, and vision assessments.[2]
-
Investigations:
In some cases, the clinical phenotype will clearly point to a cause for the LD (e.g. Down’s syndrome) and little further investigation will be necessary.
Some examples of these include:
- Blood tests for FBC, U&Es, liver function, renal function, clotting, thyroid function, glucose, and lipids;
- infection screening or serology (blood, urine, occasionally CSF) for rubella, toxoplasmosis, HIV, CMV, EBV, HSV, and syphilis;
- metabolic screening of blood for inborn errors of metabolism;
- genetics: karyotyping, single gene disorder testing (e.g. fragile X DNA testing);
- imaging of dysmorphia or abnormalities seen on physical examination, e.g. X-rays, CT/MRI (especially cranial);
- ECG, echocardiography;
- EEG, visual evoked potentials, muscle biopsy.[2]
[/vc_column_text][/vc_tta_section][vc_tta_section title=”Management” tab_id=”1548501377839-4ee707df-eb67″][vc_column_text]
The management of a patient with LD should be as for any other complex patient, with special attention to the psychological and social needs of the family. [2]
Table 1.5 Goals of service provision for a person with learning disability:
| ‘Normalize’ the person’s life |
| Recognize individual needs |
| Develop abilities |
| Offer choice also involve the patient in management decisions |
| Provide the best possible care for physical and psychiatric problems |
| Support the family or carers |
Table 1.6 Components of a service for people with learning disability:
Social and psychological |
| Support for family at home; additionally, respite admissions |
| Education, training, also occupation |
| Social activities |
| Accommodation |
| Help with financial also other problems |
Medical |
| Treatment of physical disorders |
| Management of challenging behaviour |
| Behavioural therapy |
| Cognitive behavioural therapy |
Treatment of psychiatric disorders |
| Psychological treatments |
| Pharmacological treatments |
-
Social interventions
-
Help for families i.e.:
As explained above, parents need continuing psychological support and help with practical matters such as day care during school holidays, babysitting, or arrangements for family vacations. The volunteers can play a valuable part in the arrangements. The Internet is now providing a huge support base for parents with children suffering from rare conditions. [2]
-
Education i.e.:
Extra education and training before school age (compensatory education) helps children with LD to realize their potential. When the normal school age is reached, the least disabled children can be educated in a special class in an ordinary school. It has the disadvantages of lack of special teaching skills and the risk that the child may not be accepted by more able children. The period after leaving school is difficult for people with LD and they need a lot of help from their general practitioner and the specialist services. It is important to review the prospects for employment, suitability for further training, and requirements for day care. At this stage of life.[2]
-
Training and work i.e.:
Most people with mild learning difficulties are capable of work and benefit from appropriate training. However, except at times of full employment, suitable work may not be available and sheltered occupation is needed. [2]
-
Social activities i.e.:
People with LD need to develop leisure activities appropriate to their age, ability, and interests. Whenever possible this should be achieved by joining activities arranged for able people, but clubs and day centres for the disabled are also needed. Leisure activities need to be arranged as part of the program of the training centres that provide sheltered work.[2]
-
Accommodation i.e.:
Many people with LD live with their families. For the rest, a variety of accommodation is required ranging from ordinary housing to staffed hostels. A useful intermediate level of supervision is provided in a ‘core and cluster’ system in which several group homes are sited near to a central staffed unit.
When parents grow old and can no longer care for their disabled son or daughter, special accommodation is required.[2]
-
Help with financial and other practical problems i.e.
People with LD may need help in managing their money, dealing with forms, regulations, and other problems of daily life. In most developed countries there are various social benefits available for people with functional needs. Special equipment for the home is also available and occupational and physiotherapists can be very helpful in arranging this. [2]
Medical and psychological interventions in Learning Disorder:
-
General medical services i.e.:
It is good practice to keep a register of these patients and arrange regular health checks. Basic physical problems (e.g. toothache, hay fever) are a great source of behavioural disturbance, and should be actively sought and aggressively managed.[2]
-
Treatment of challenging behaviour i.e.:
The most important step in treating challenging behaviour is to identify the cause; if possible, this is then removed/treated.
1. Behavioural therapy:
Behavioural techniques are very helpful in teaching basic self-care skills and establishing normal patterns of behaviour. Eating, sleep, and disobedience problems respond well to simple parenting skills. It can be used in people without verbal skills, which is a benefit over most other treatments.
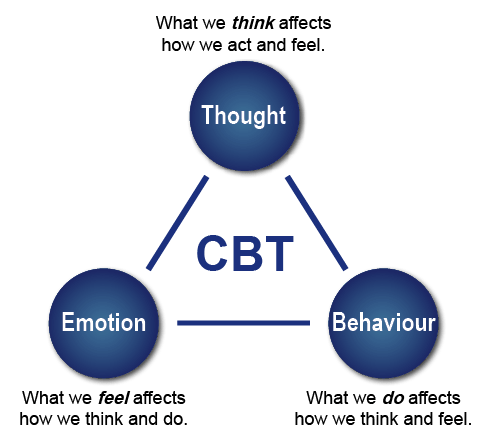
2. Cognitive behavioural therapy:
CBT can successfully use in people with mild to moderate LD. Anger management, aggression, interpersonal skills, low self-esteem, also problem-solving skills can all treat with CBT in LD. It has been found that CBT for LD actually works best when delivered in a group format.[2]
-
Psychodynamic therapy and counselling:
The principles of a comprehensive analysis can be very useful in treating patients with a LD who have suffered emotional abuse also severe psychological disturbance at an early age. [2]
Treatment of psychiatric disorder:
Treatment of mental disorder among people with LD is similar to that of the same disorder in a patient of normal intelligence.
Psychopharmacological treatments are widely use in LD, partly because the patients frequently have physical disorders (e.g. epilepsy) which are independent indications for them. Whilst medications do have a role to play in relieving specific symptoms and behaviours, they should not use without a good indication.
1. Antipsychotic:
Antipsychotic drugs are use for psychosis, challenging behaviour (especially in autism, self injury, and social withdrawal), tic disorders, and in severe mood disorders. Patients with LD are more prone to the metabolic side effects of atypical antipsychotics (e.g. weight gain, metabolic syndrome) and should carefully monitor.
2. Antidepressants:
Depression, OCD, anxiety disorders, and self-injury all respond well to standard antidepressant therapy.
3. Mood stabilizers
They use in the treatment of bipolar disorder and severe depression, and are a particularly good choice in patients with co-morbid epilepsy.
4. Stimulants
They now widely use to tackle hyperactivity and ADHD, and there is some evidence that they can improve behaviour more globally (improving eating, sleep, and mood).
5. Opiate antagonists:
There is a hypothesis that opioid excess may underlie autism and self-injury, and naltrexone has use to treat both these conditions. There is little evidence that it improves symptoms in autism, but it does reduce the frequency and severity of self-injury. [2]
[/vc_column_text][/vc_tta_section][vc_tta_section title=”Homeopathic treatment” tab_id=”1548501578761-dbd75685-69cd”][vc_column_text]
Homeopathic treatment
Homeopathy has excellent success rate in this treatment. Homeopathy will consider entire symptoms of your child whether related or not to learning disabilities also will treat him or her constitutionally.
With effective homeopathic treatment for learning Disabilities, you will notice concrete changes such as the following i.e.:
- Improved confidence level in child.
- Better academic performance.
- Reduced levels of frustration also helplessness in your child.
- Distinct change in your child’s learning skills.
- Handwriting will become more legible with less spelling mistakes.
- Gradually your child will enjoy reading, writing also solving mathematics problems.
- Better development of social and interpersonal skills in kids.
Moreover, Homoeopathic treatment for Learning Disabilities also helps in preventing the relapse of the condition. Homoeopathic treatment for Learning Disabilities provides complete holistic wellbeing to the patient and assists recovery in the safest and most natural way. [3]
Homeopathic treatment for Learning Disabilities is natural, safe and without any side-effects. It is a patient-oriented science with vast range of medicines to treat Learning Disorder efficiently.
Few of our amazing remedies in Homeopathic treatment for learning disabilities include:
-
Baryta Carbonica:
Excellent remedy especially for Learning Disorder in shy and timid kids who are greatly averse to meet strangers. Associated poor memory. They have great fear of giving wrong answer. They are less mature and look lost. Confusion is mark. Also they have tendency to take cold easily.
-
Calcarea Carbonica:
Generally, great remedy for kids who are apprehensive and forgetful. In detail, They are bad towards evening. These kids are obstinate and slow. Milestones are delay. Lastly, Such children usually have craving for indigestible things like chalk, coal etc. They like eggs, salt also sweets.
-
Calcarea Phosphorica:
Suits effectively children with Learning Disorder who are tall, lean with little energy. They are forgetful, frustrat and suffers from difficult dentition. They crave non-vegetarian food especially meats.
Have a look at some of the remedies used for the homeopathic treatment for learning disability. [3]
The remedy abbreviations with,
- 4 marks- most effective,
- 3 marks- quite effective,
- 2 marks- less effective,
- 1 mark- least effective.
LEARNING: Difficult: 1Acon, 1Aeth, 4AGAR, 1Agn, 1Aids, 1Alch, 1Ambr, 3Anac, 1Androc, 1Aq-mar, 3Ars, 1Ars-i, 3Asar, 4BAR-C, 3Calad, 1Calc, 1Calc-p, 1Canth, 1Caps, 1Carb-ac, 1Carb-v, 1Carc, 1Caust, 1Cham, 1Chap, 1Choc, 4COCC, 1Colch, 1Con, 1Cycl, 1Dpt, 1Euon,3Excr-can, 1Falco-p, 3Gels, 1Hell, 1Hep, 2Hoch, 1Hydrog, 1Ign, 1Joan, 3Kali-c, 1Kali-p, 1Kali-sil, 1Lyc, 1M-arct, 1Mag-p, 1Merc, 1Mez, 3Mur-ac, 1Nat-c, 1Nat-m, 3Nit-ac, 1Nux-m, 3Olnd, 1Op, 1Ph-ac, 1Phol-p, 3Phos, 1Phyt, 1Pter-a, 4PULS, 3Ran-b, 1Rhus-t, 1Sars, 4SEP, 1Sil, 2Sol,4STANN, 3Staph, 1Stram, 3Sulph, 1Tanac, 1Tax-br, 1Teg-a, 1Thuj, 1Thul, 1Toxo, 1Tung, 1Uran, 4ZINC,3Zing
LEARNING, DISABILITIES, STUDYING, READING: Understanding, difficult: 1Agn, 2Ail, 1Alum, 2Anac, 2Bapt, 3Bar-c, 3Carc, 1Cocc, 2Gels, 2Hell, 1Kali-p, 1Lyc, 1Nat-c, 2Nux-m, 1Olnd, 2Op, 2Ph-ac, 1Phos, 1Plb, 1Xero,2Zinc
MATHEMATICS,CALCULATING: Inept for: 1Acon-f, 4AIL, 1Alco, 2Alum, 3Am-c, 3Ambr,2Amet, 1Anh, 1Arb-m, 1Arg-s, 1Aur, 1Bell, 1Calc, 1Cand-a, 1Carb-v, 1Caust, 1Chin-s, 1Chlam-t, 1Cocain, 1Con, 3Crot-h, 1Graph, 3Lac-eq, 2Lac-h, 1Lac-m, 1Lach, 1Lamp-c, 2Lyc,3Merc, 1Mosch, 1Nat-c, 1Nat-m, 4NUX-V, 1Ph-ac, 1Plb, 1Psil-s, 3Psor, 1Rhus-t, 1Sop-m, 1Staph, 3Sumb, 1Syph, 1Tax, 1Thal-s, 3Thuj, 1Tung, 1Unc-t [3][/vc_column_text][/vc_tta_section][vc_tta_section title=”FAQ” tab_id=”1548501662642-2598d5ef-bbae”][vc_column_text]
Frequently Asked Questions
What is Learning Disabilities?
The term learning disabilities (LD) and the alternative phrase mental retardation denote an irreversible impairment of intelligence originating early in life which is associated with limitations of social functioning.
Homeopathic Medicines used by Homeopathic Doctors in treatment of Learning Disabilities?
- Baryta Carbonica
- Calcarea Carbonica
- Calcarea Phosphorica
What causes Learning Disabilities?
- Family history and genetics
- premature birth
- Psychological trauma
- Physical trauma
- Environmental exposure
What are the symptoms of Learning Disabilities?
- Problems pronouncing words
- Trouble finding the right word
- Difficulty rhyming
- Trouble learning the alphabet, numbers, colors
- Difficulty following directions or learning routines
- Trouble learning the connection between letters and sounds
- Unable to blend sounds to make words
- Confuses basic words when reading
- Slow to learn new skills
Give the types of Learning Disabilities?
- Learning disabilities in reading (dyslexia)
- Learning disabilities in math (dyscalculia)
- Learning disabilities in writing (dysgraphia)
- Learning disabilities in motor skills (dyspraxia)
- Learning disabilities in language (aphasia/dysphasia)
- Auditory and visual processing problems
[/vc_column_text][/vc_tta_section][vc_tta_section title=”Reference” tab_id=”1548502686445-2397cc97-c1c5″][vc_column_text]
- https://www.helpguide.org/articles/autism-learning-disabilities/learning-disabilities-and-disorders.htm
- Psychiatry, Fourth Edition – Oxford Medical Publications -SRG-by John Geddes, Jonathan Price, Rebecca McKnight
- https://www.welcomecure.com/diseases/learning-disabilities/homeopathic-treatment
[/vc_column_text][/vc_tta_section][/vc_tta_tour][/vc_column][/vc_row]