Classification of Psychiatric Disorders:
In psychiatry, as in the rest of the medicine, Classification of Psychiatric Disorders is needed for three main purposes:
1. To enable clinicians to communicate with one another about their patients symptoms, prognosis and treatment.
2. To ensure that research can be conducted with comparable groups of patients.
3. To enable epidemiological studies as a basis for research and planning services.
Systems of classification of Psychiatric Disorders:
There are mainly two systems of classification which are described in brief below.
- DSM IV
- ICD 10
Psychiatric Disorders also classified according to HOMEOPATHIC.
What Is DSM V Classification of Psychiatric Disorders ?:
1.Classification of Psychiatric Disorders are done by the diagnostic and statistical manual of mental disorders, more commonly known as the DSM, currently in its 5th edition hence DSM V.
2. It is published by the American Psychiatric Association and categorizes mental disorders for both children and adults.
3. It also lists known causes of these disorders, statistics in terms of gender, age at onset, and prognosis as well as some research concerning the treatment options and most appropriate approaches.
4. It has become a standard for mental health professionals to use the DSM V on a routine basis in their daily practice.
5. Its to use help to have a better and common understanding of mental illnesses and potential treatments as well as communicating with others such as insurance companies.
6. Many refer to it as for any professional who makes psychiatric diagnoses in the United States.
7. Only a trained and licensed clinician such as a psychologist or psychiatrist can accurately diagnose psychiatric disorders since this requires a thorough understanding of the complex and overlapping psychiatric symptoms
8. Psychiatric disorders are classified according to their predominant symptom.
9. For example, depression, dysthymic disorder and bipolar disorder all have a disturbed mood pattern as their main feature and therefore all of these are classified under Mood Disorders.
10. The DSM uses a multiaxial or multidimensional approach to diagnosing because rarely do other factors in a person’s life not impact their mental health. It assesses five dimensions as described below:
Axis I: Clinical syndromes:
This is what we typically think of as the diagnosis (e.g., depression, schizophrenia, social phobia).
Axis II: Developmental disorders and personality disorders:
In general, Developmental disorders include autism and mental retardation, disorders which are typically first evident in childhood. Moreover, Personality Disorders are clinical syndromes which have a more long lasting symptoms also encompass the individual’s way of interacting with the world. Besides this, They include paranoid, antisocial, and borderline personality disorders.
Axis III: Physical conditions
which play a role in the development, continuance, or exacerbation of Axis I and II Disorders: Physical conditions such as brain injury or HIV/ AIDS that can result in symptoms of mental illness are included here.
Axis IV: Severity of psychosocial stressors:
Events in a person’s life, such as death of a loved one, starting a new job, college, unemployment, and even marriage can impact the disorders listed in Axis I and II. These events are both listed and rated for this Axis.
Axis V: Highest level of functioning:
On the final axis, the clinician rates the person’s level of functioning both at the present time and the highest level within the previous year. This helps the clinician understand how the above four axes are affecting the person and what type of changes could be expected.
Classification According to DSM V:
1. Disorders usually first diagnosed in infancy, childhood or adolescence i.e.:
The DSM makes it clear that this categorization is “for convenience only” since many disorders, included in other sections, have their onset during childhood and adolescence whereas many conditions classified under this category are not diagnosed until an individual reaches adulthood. The following disorders are included in this section:
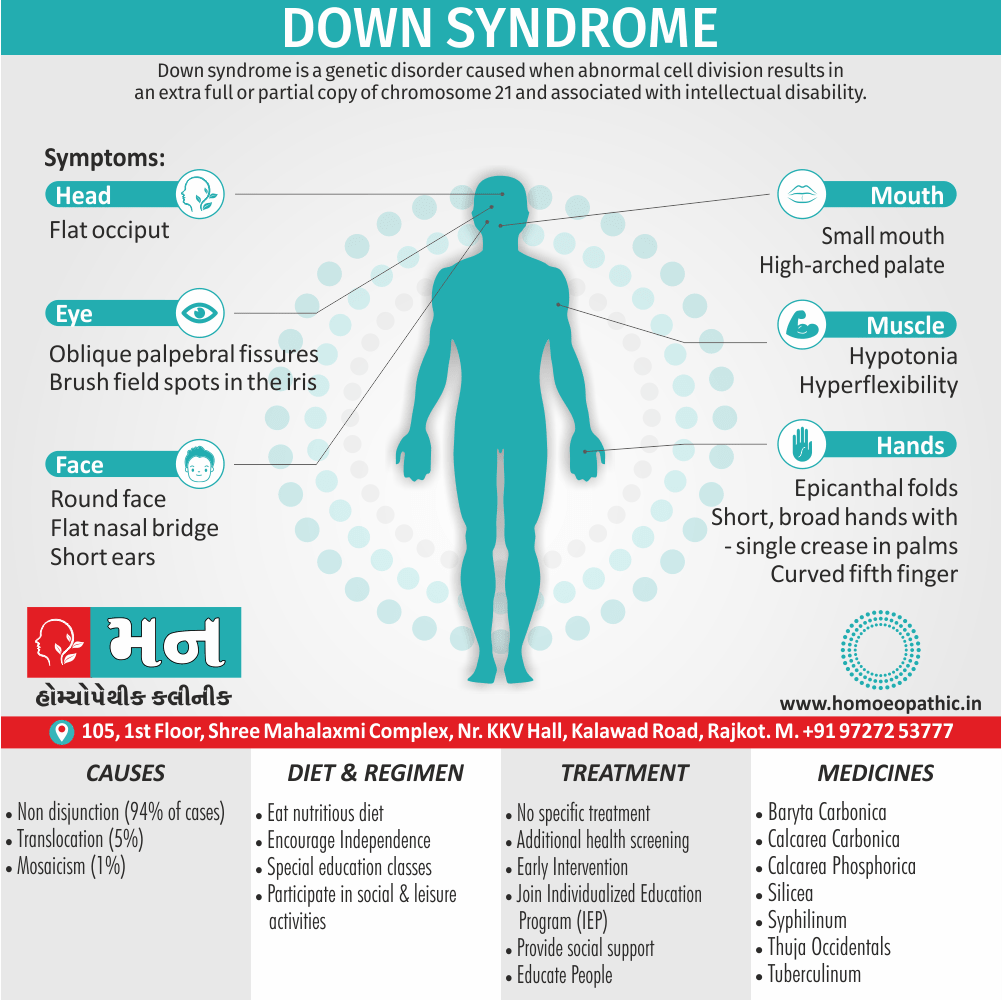
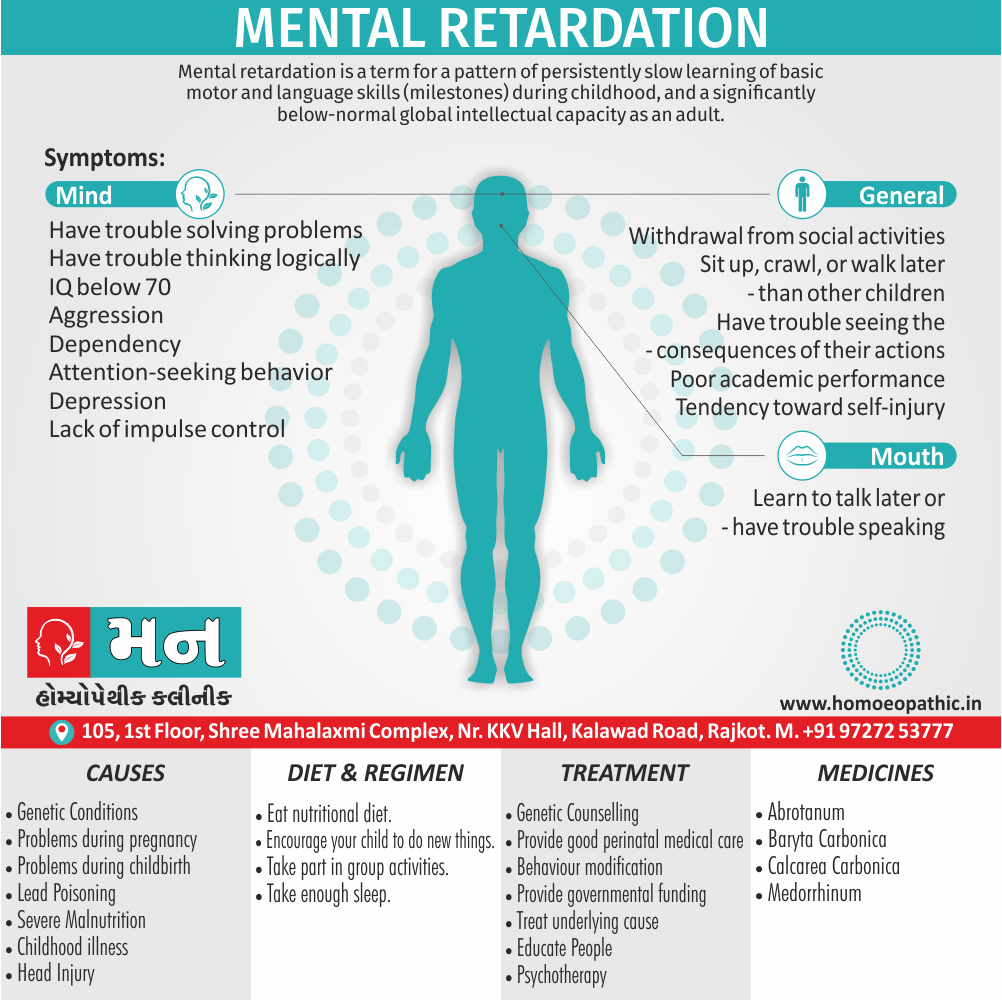
1. Mental retardation.
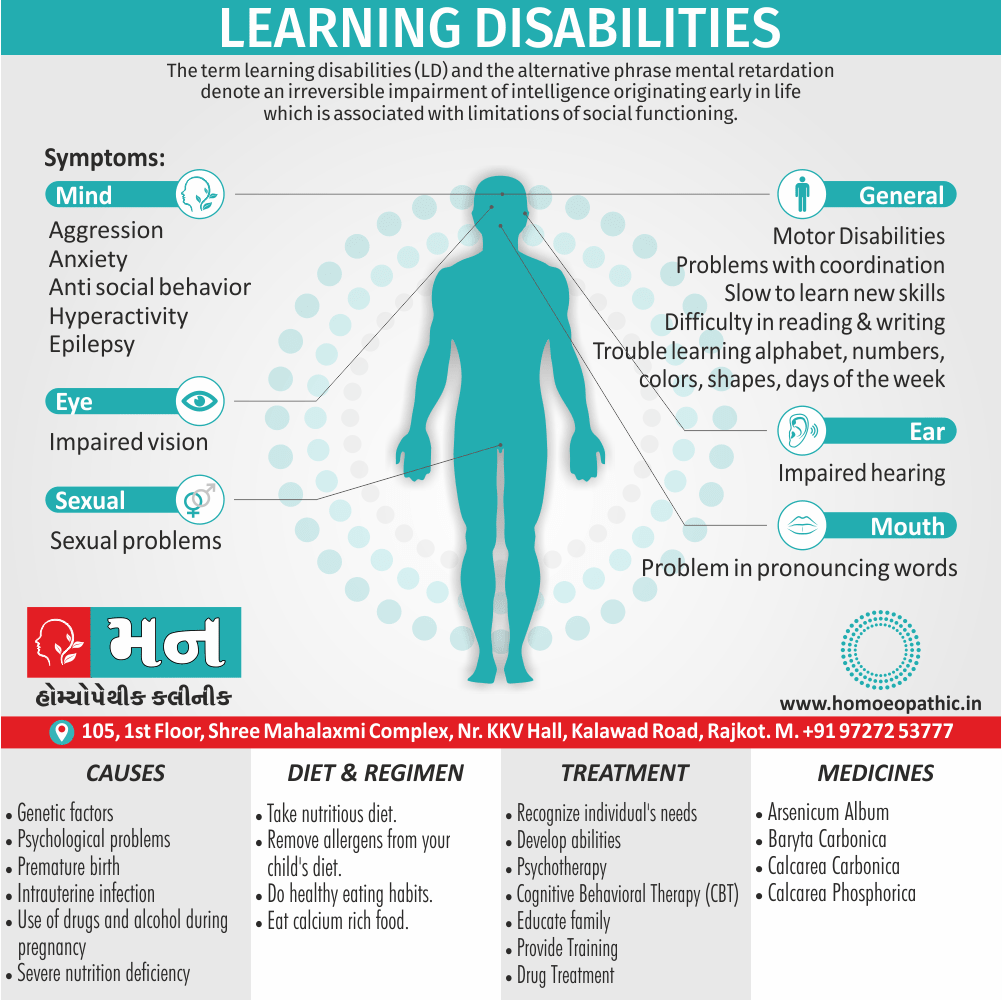
2. Learning Disorders (also commonly known as Learning Disability).
3. Motor skills disorders, communication disorders.
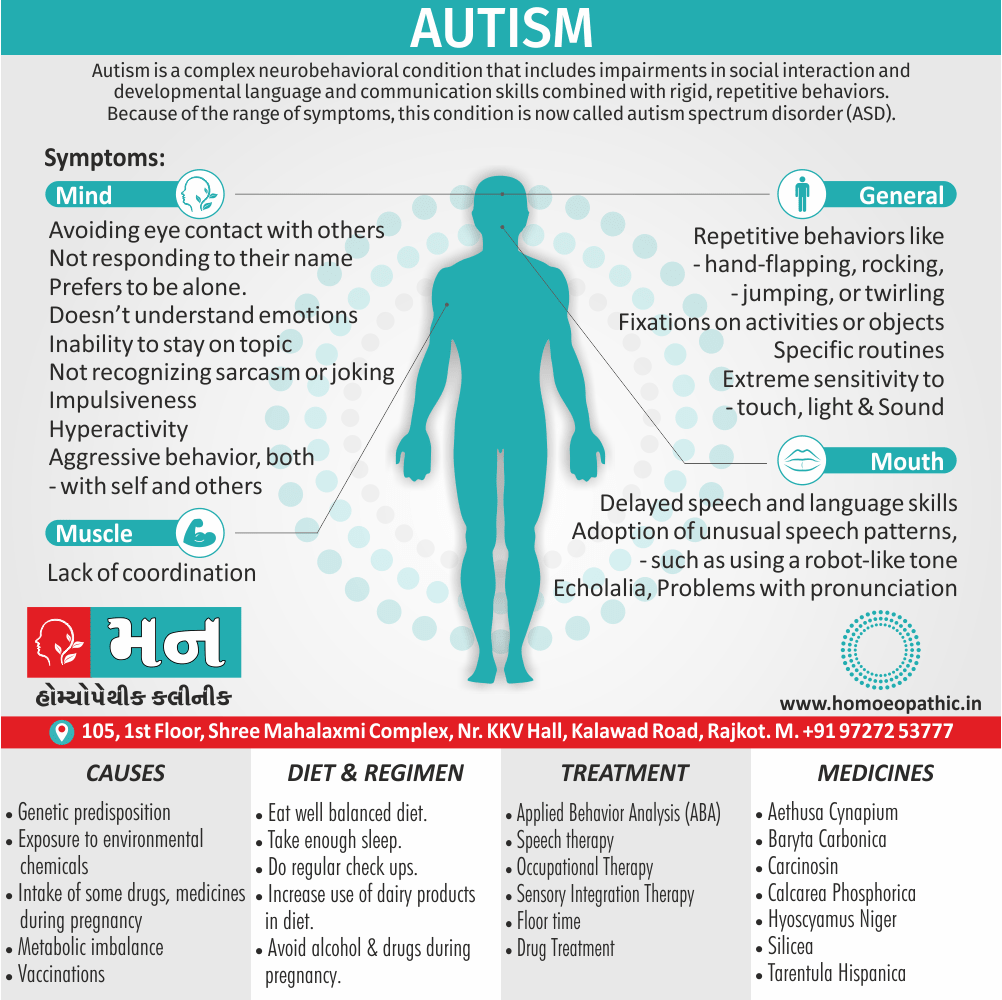
4. Pervasive developmental disorders such as autistic disorder or “Autism” and asperger disorder.
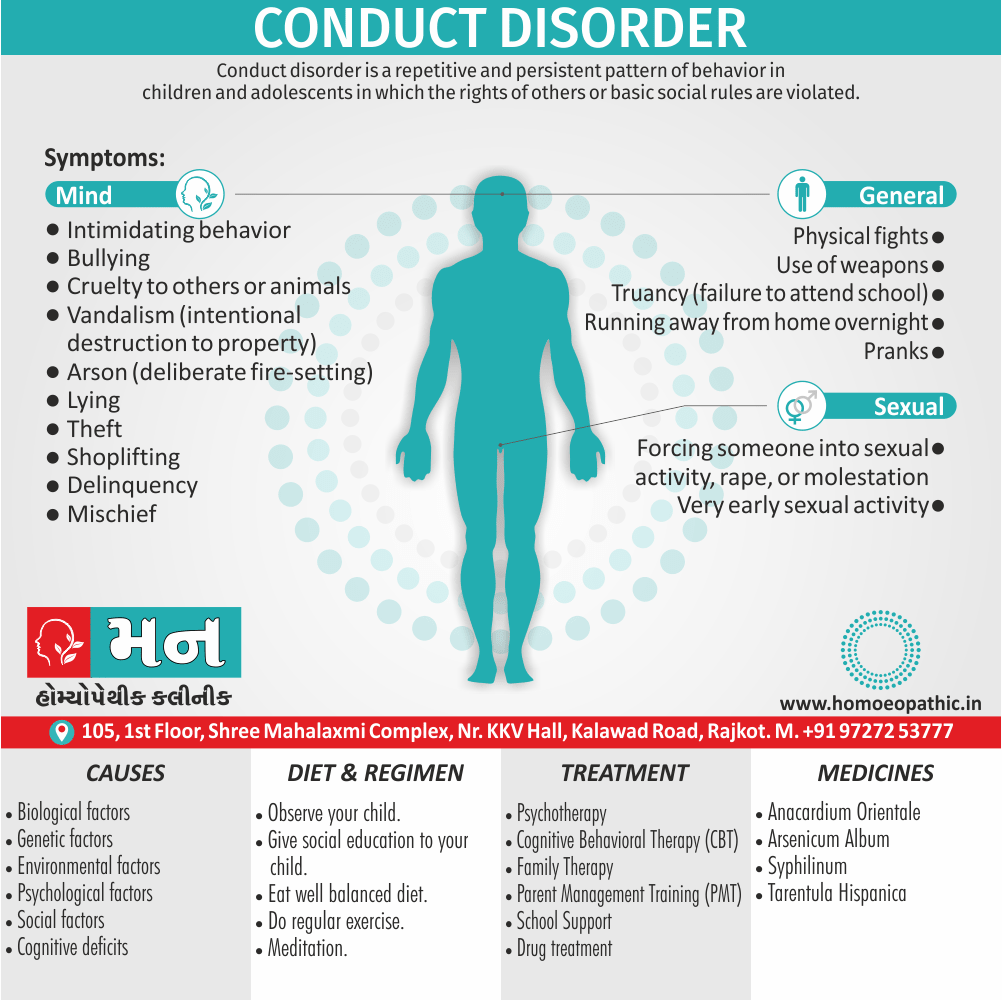
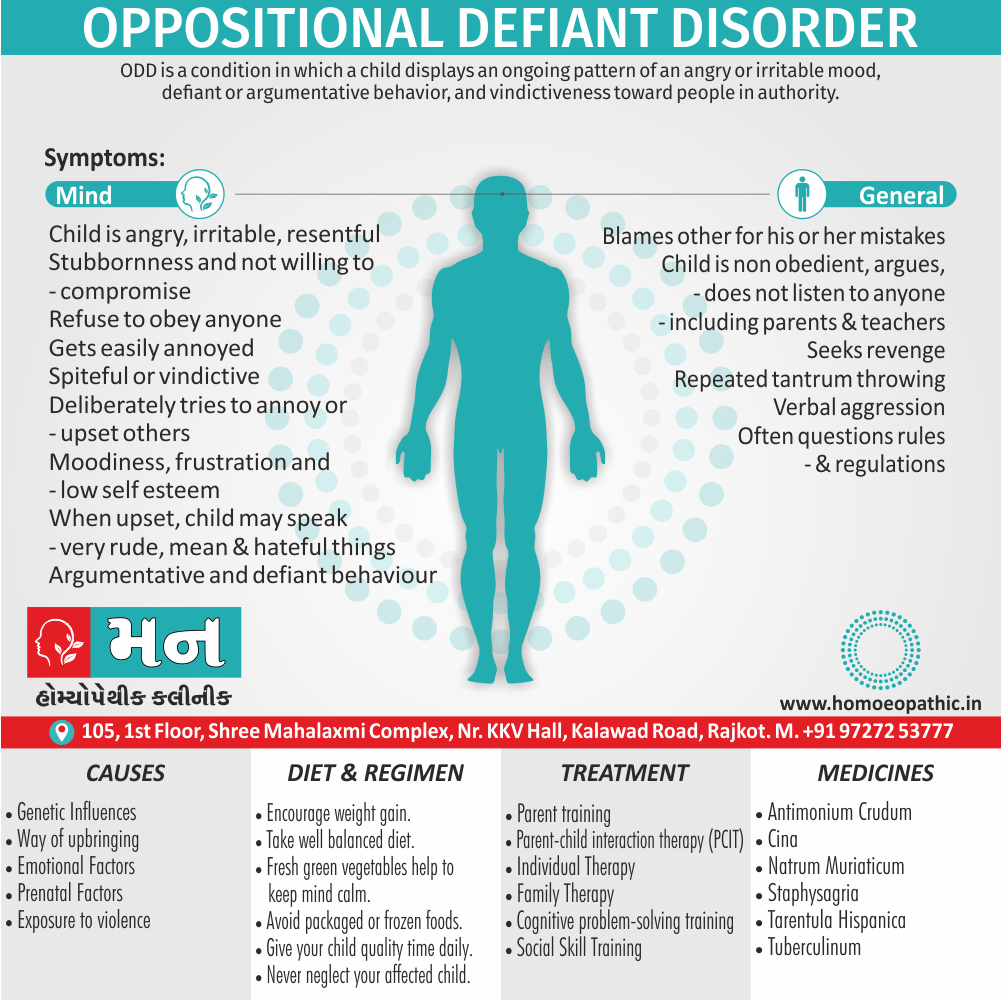
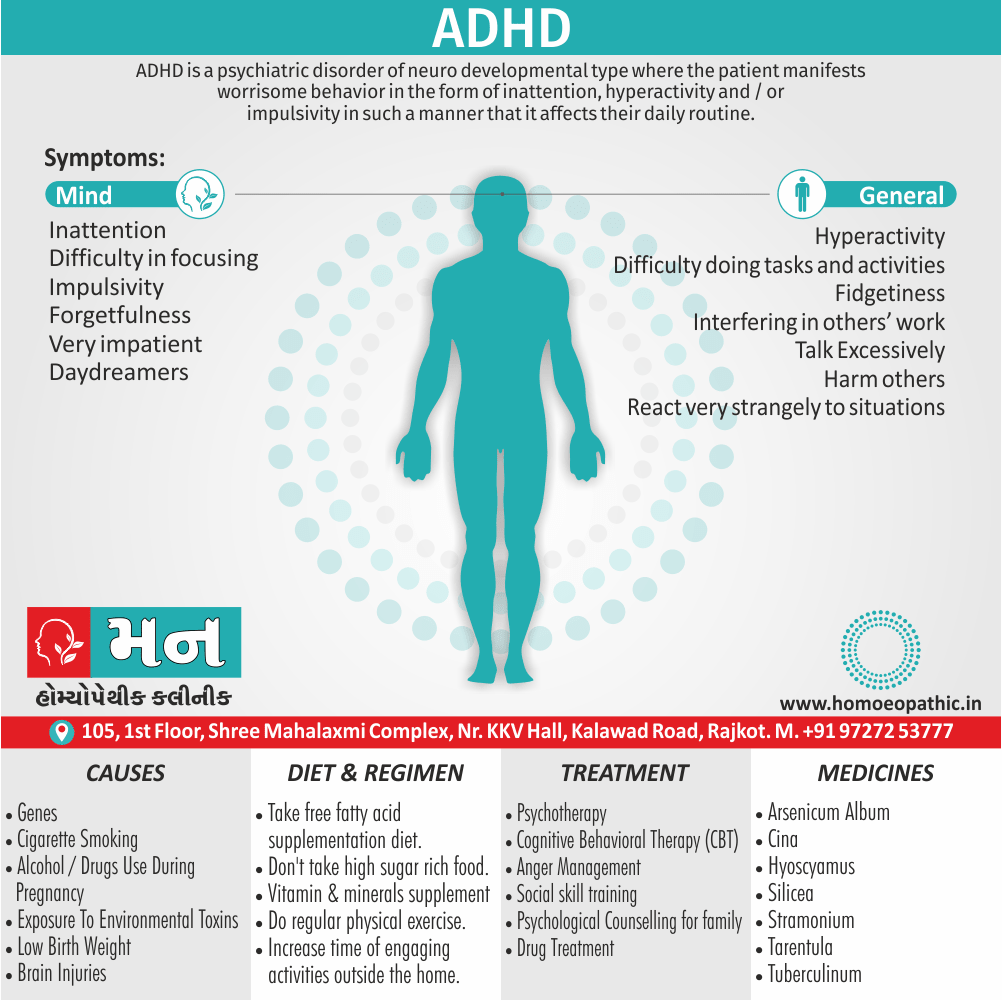
5. Attention deficit hyperactivity disorder and disruptive behaviour disorders including oppositional defiant disorder and conduct disorder.
6. Tic disorders.
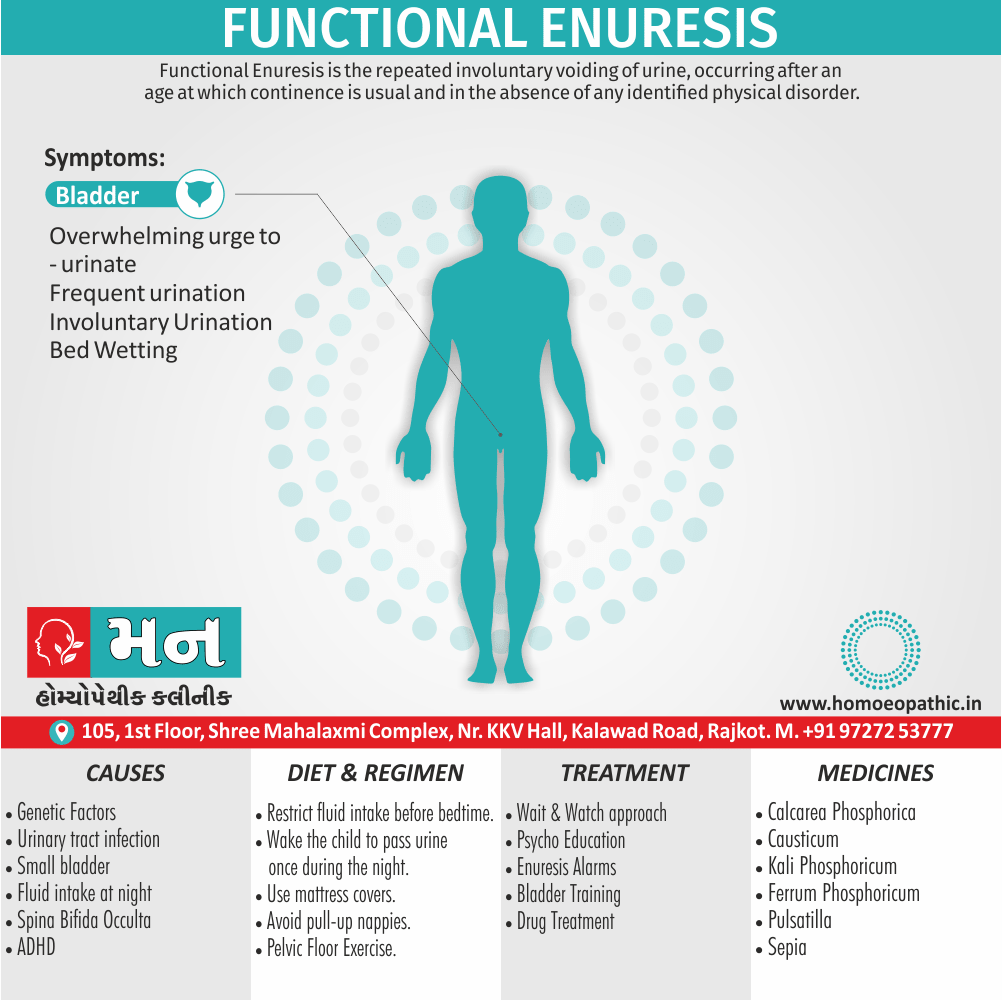
7. Elimination disorders.
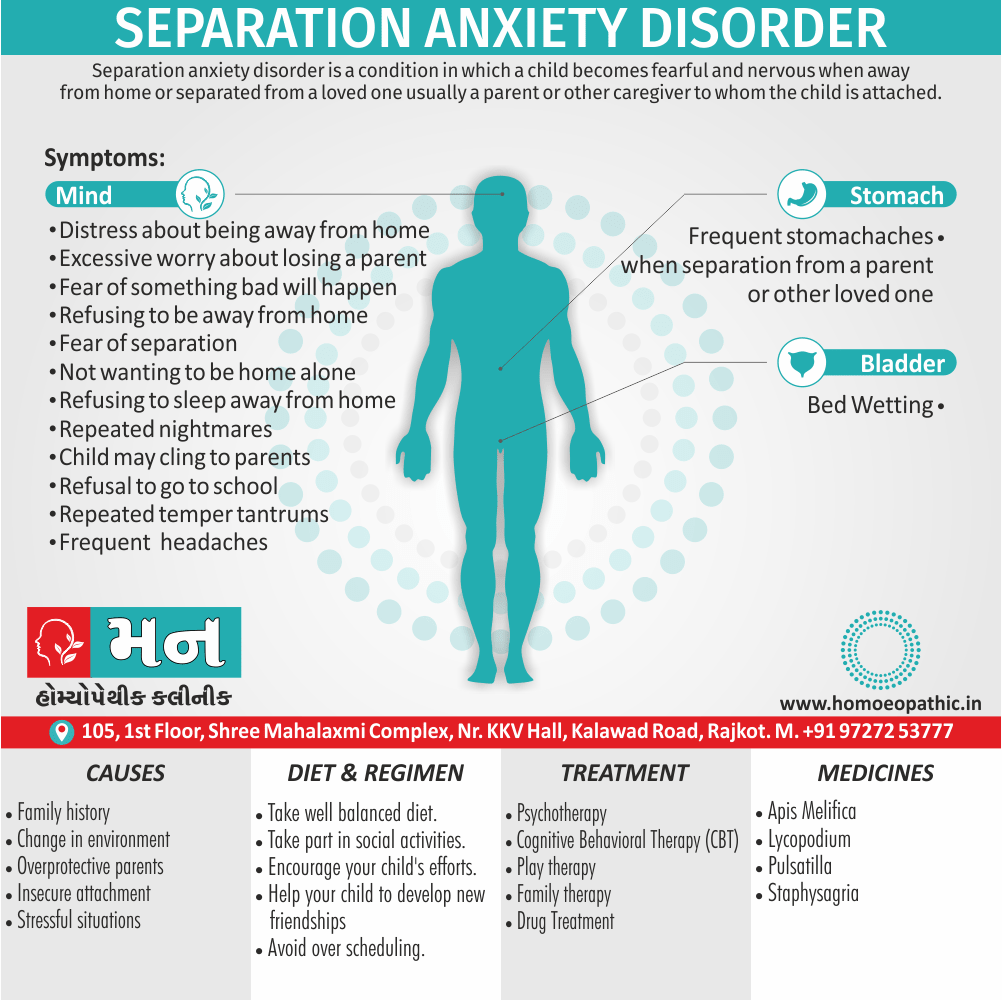
8. Separation anxiety disorder.
9. Selective mutism.
10. Reactive attachment disorder also others.
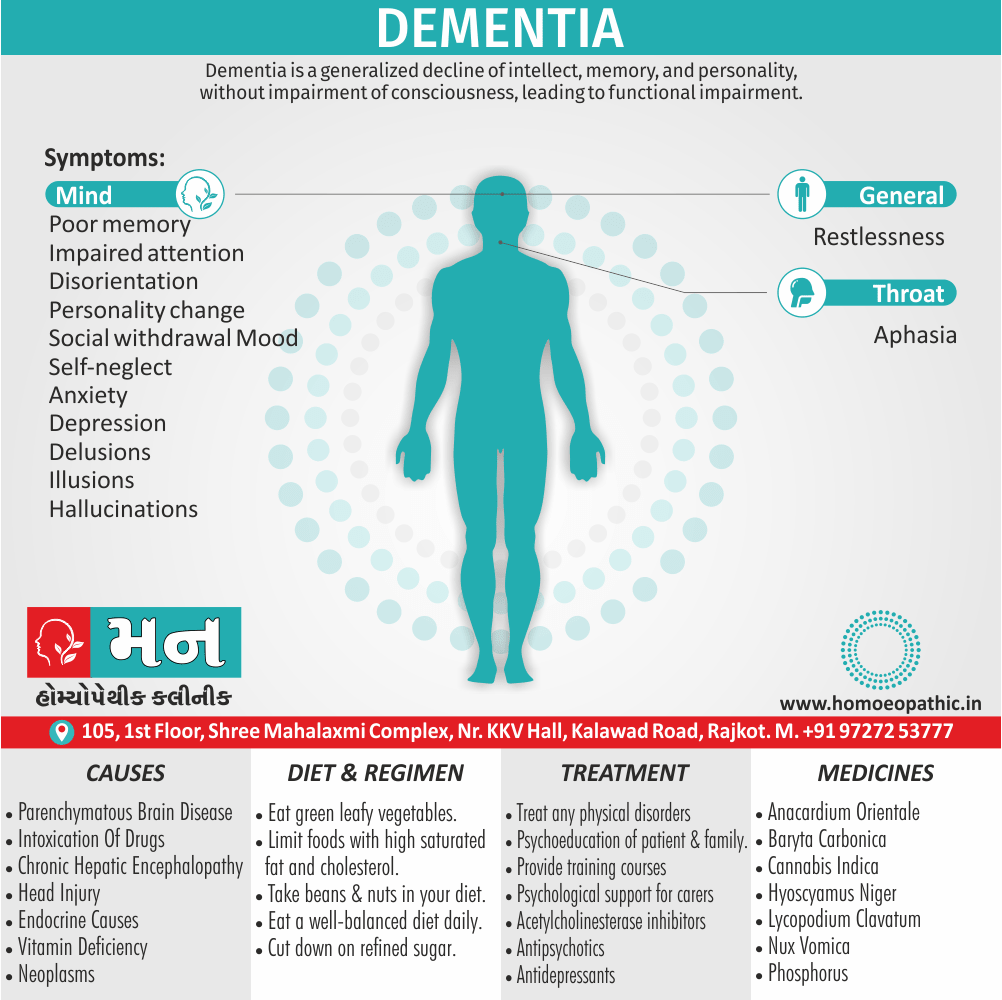
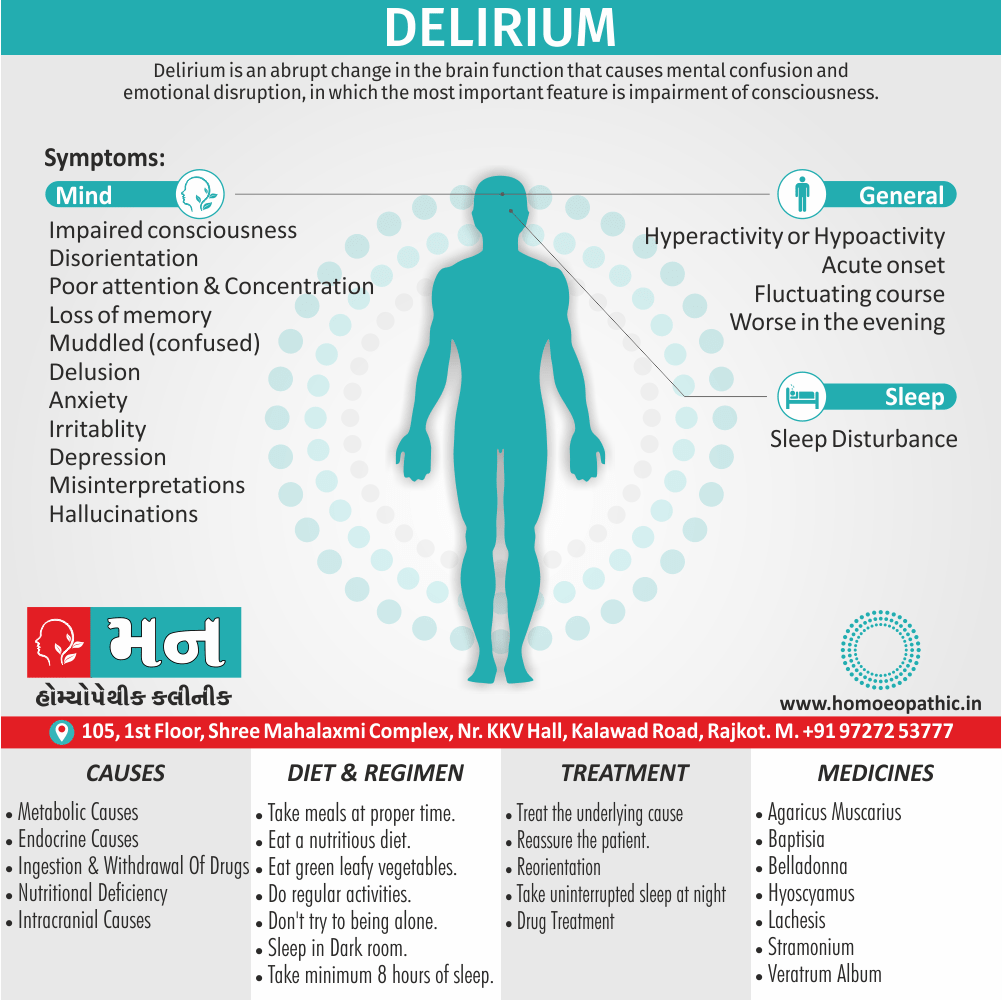
2. Delirium, dementia and other cognitive disorders i.e.:
According to the DSM IV, the main feature of various disorders in this category is “a clinically significant deficit in cognition or memory that represents a significant change from a previous level of functioning.” Examples include:
1. Delirium ( “characterized by a disturbance of consciousness and a change in cognition that develop over a short period of time”).
2. Dementia (“characterized by multiple cognitive deficits that include impairment in memory”).
3. A well-known condition in this category is dementia of the Alzheimer’s type or “Alzheimer’s disease”.
3. Mental disorders due to a general medical condition i.e.:
This category pertains to the mental symptoms that are considered to be t he direct physiological consequence of a general medical condition; examples would be
1. A personality change due to general medical condition or
2. Anxiety disorder due to a general medical condition. The main purpose of distinguishing medical conditions from mental disorders, according to the DSM IV, is to encourage thoroughness in evaluation and to enhance communication among health care providers.
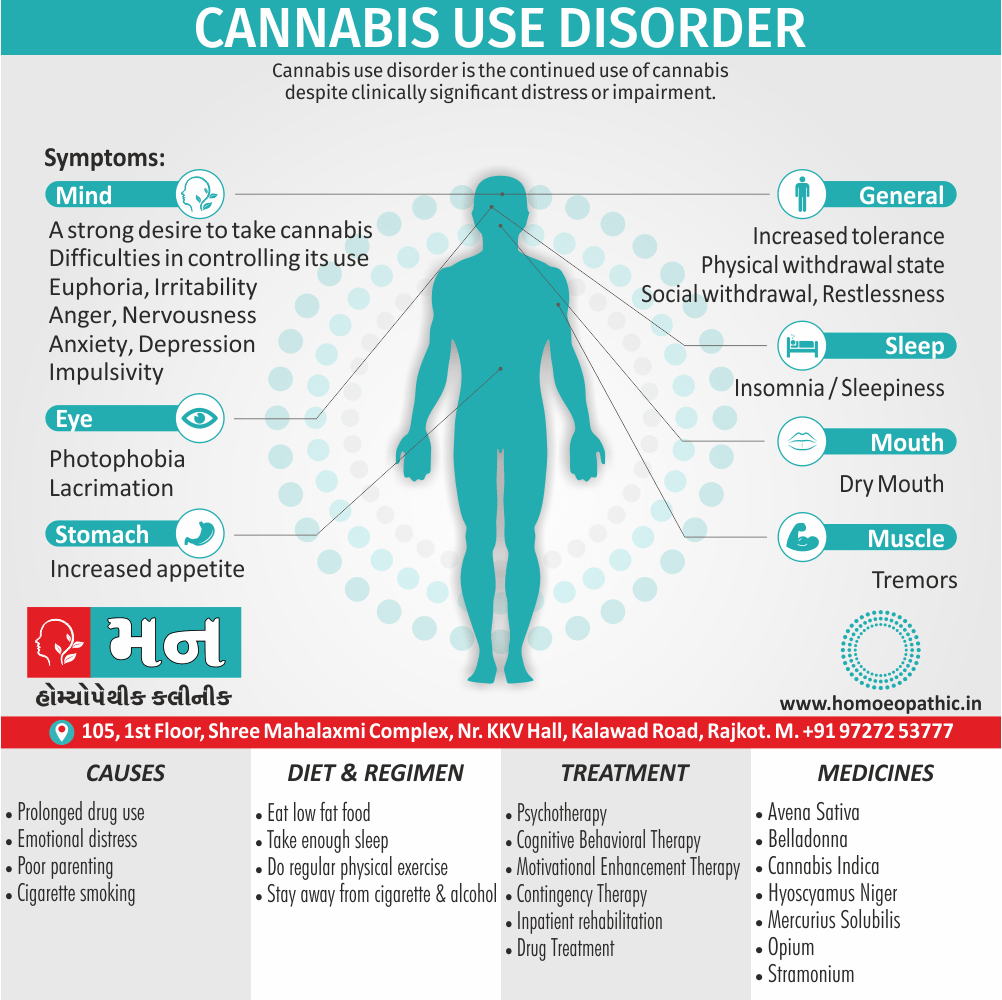
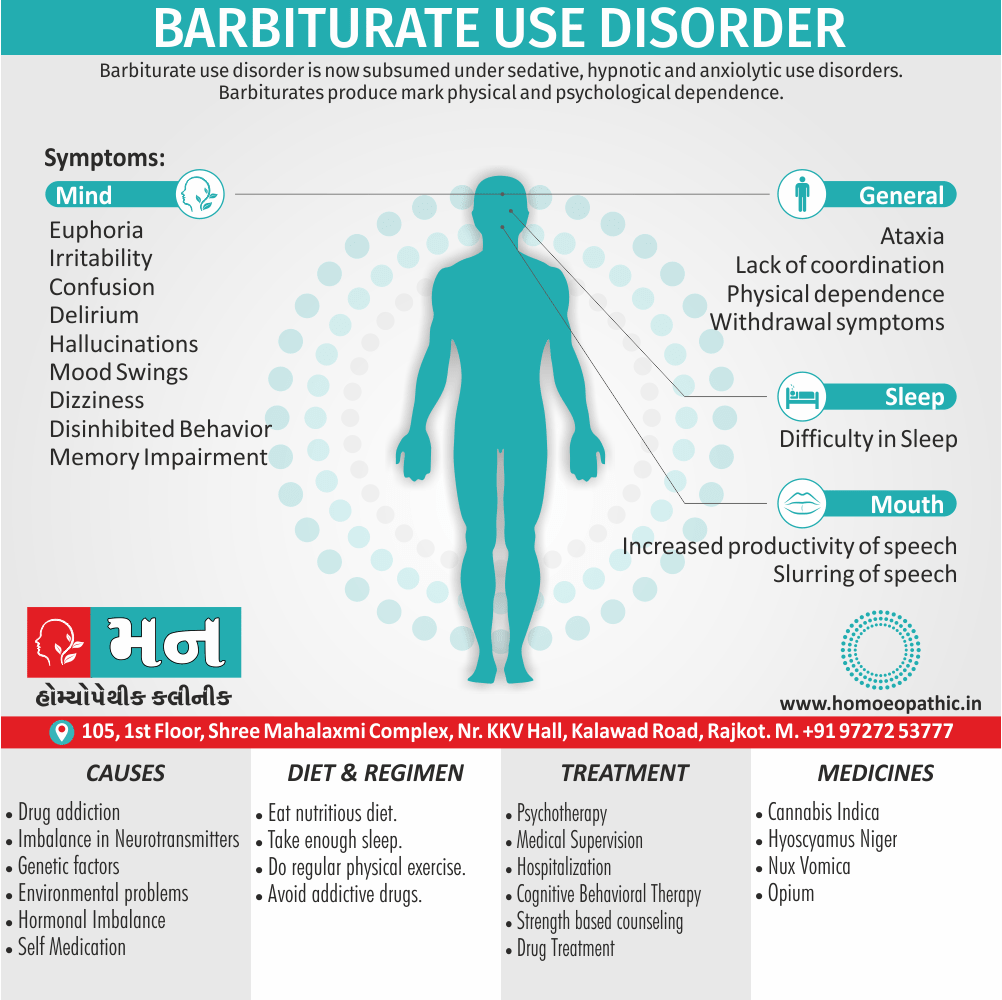
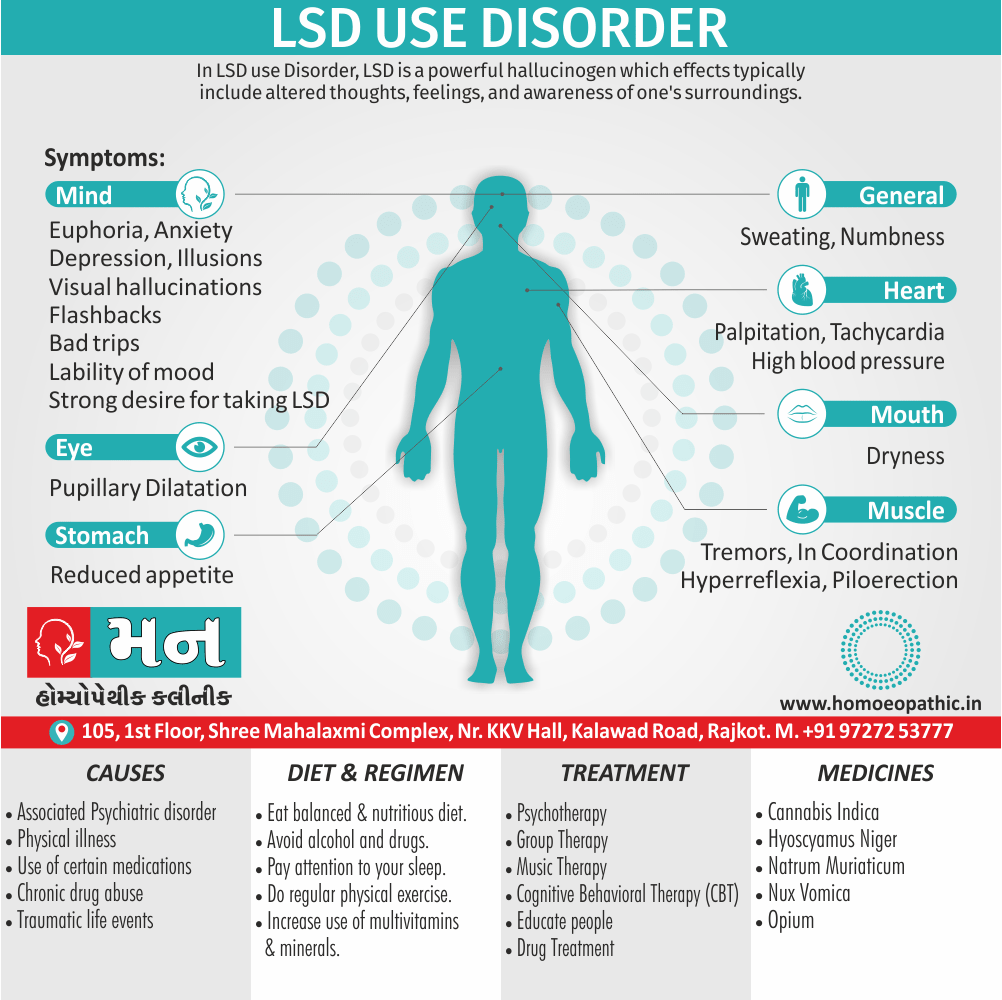
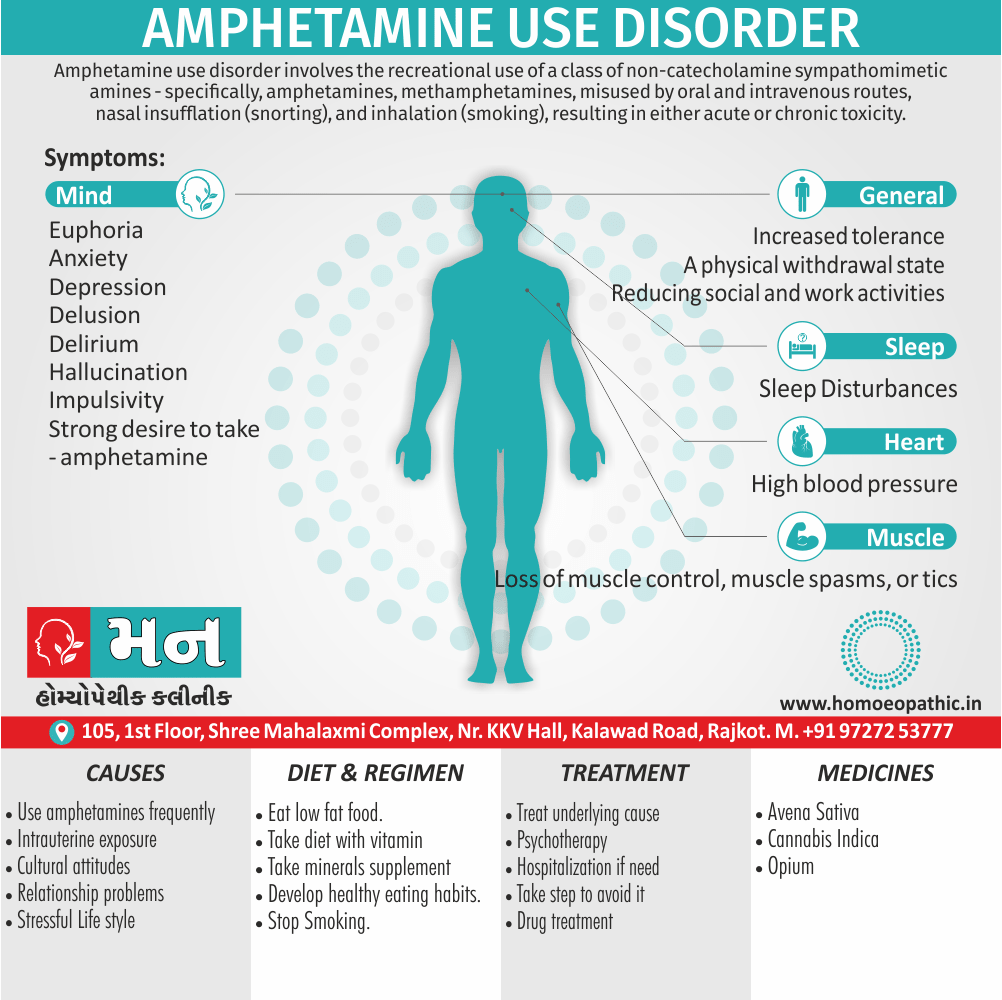
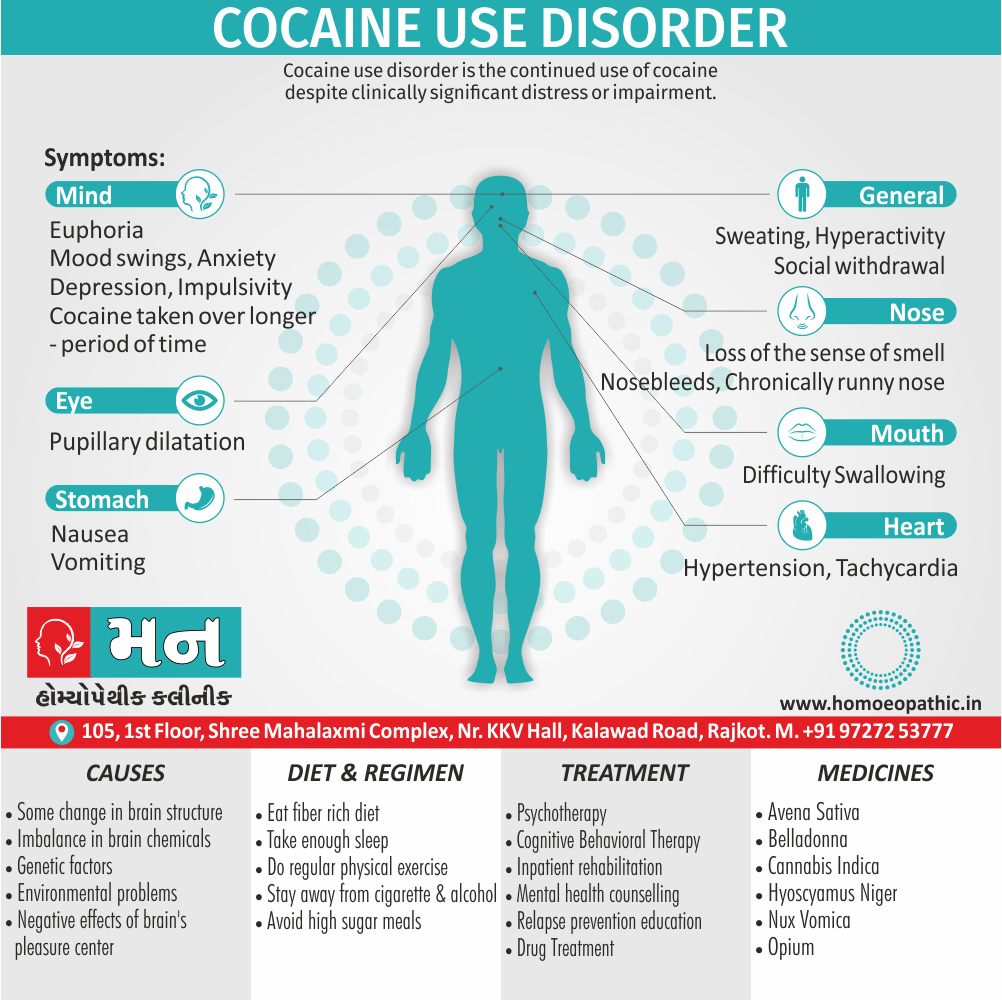
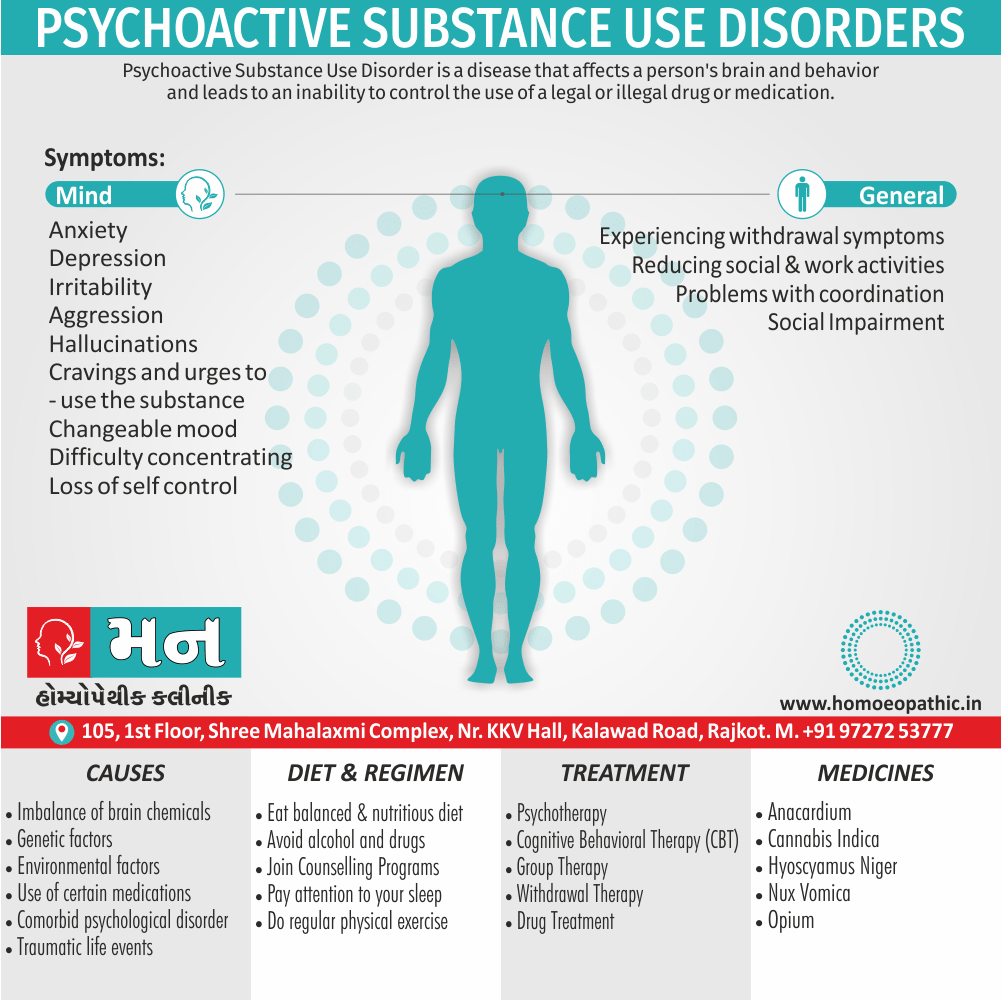
4. Substance-related disorders i.e.:
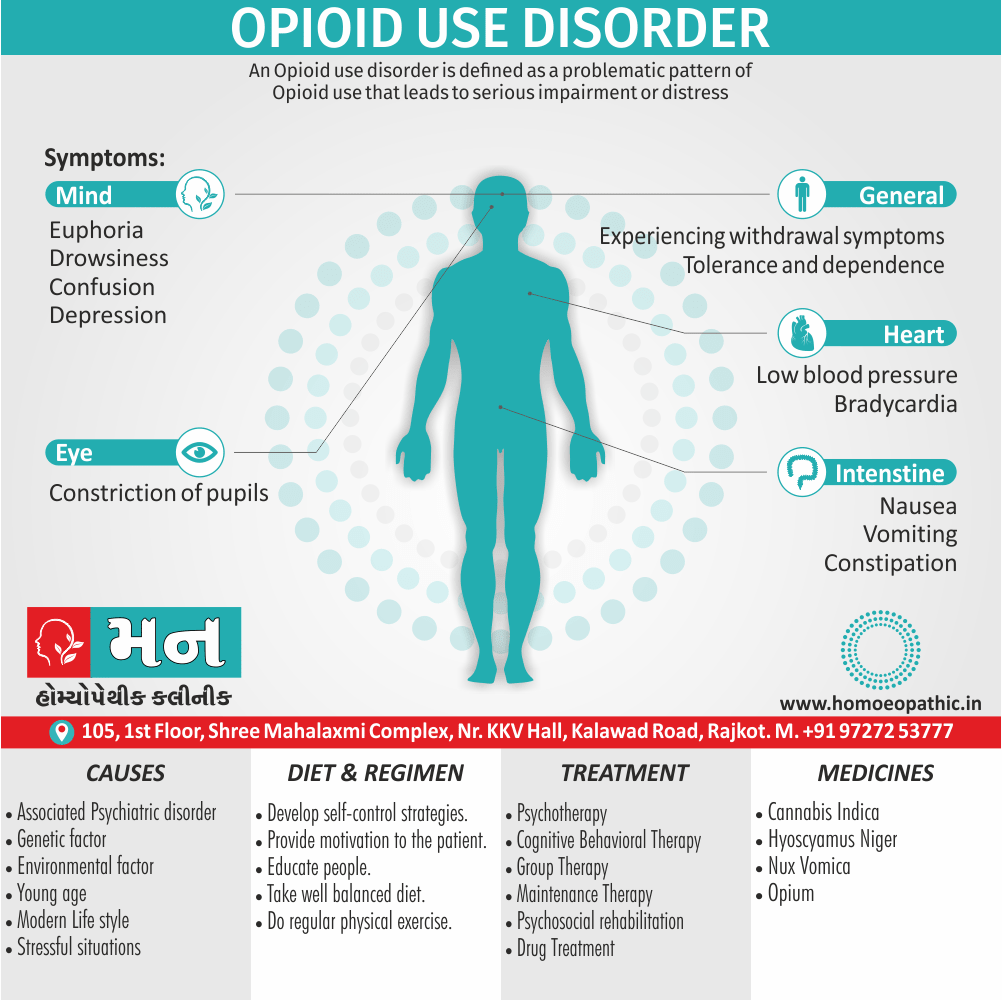
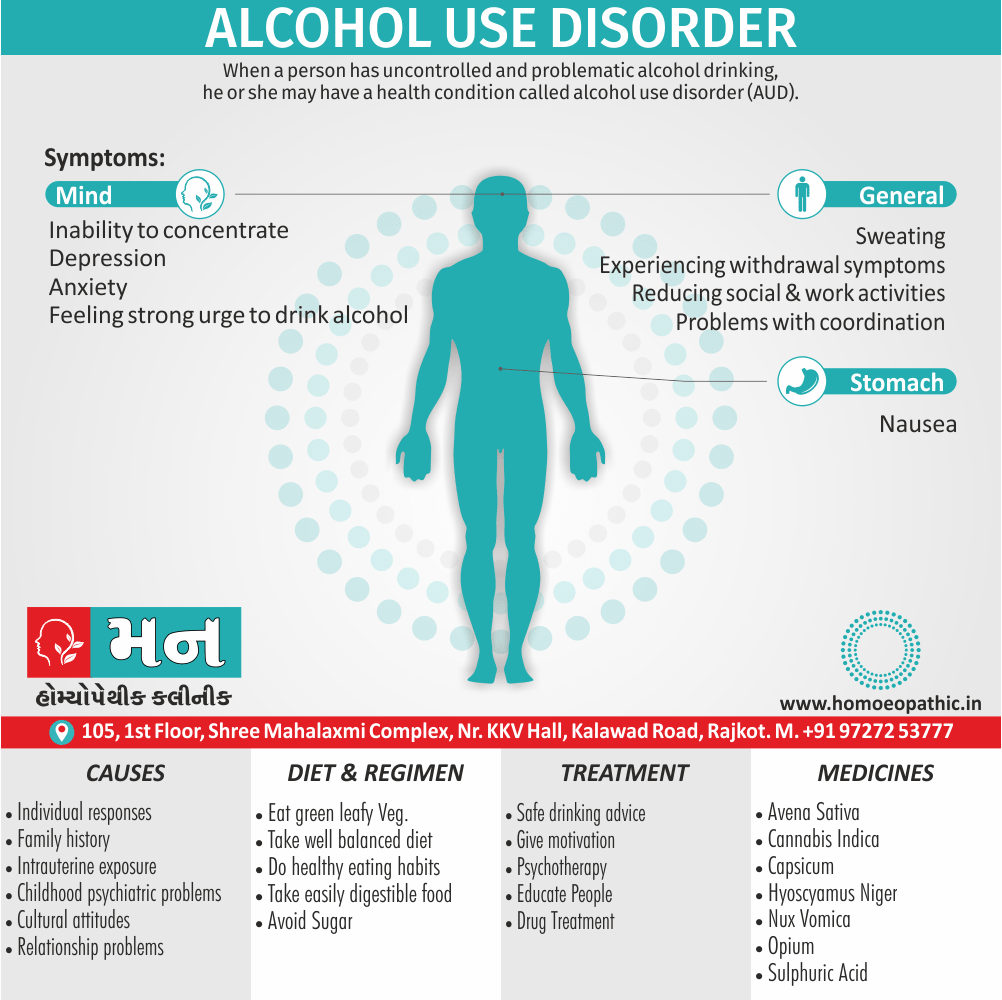
This section is about the disorders that are related to taking the drugs of abuse, including alcohol, as well as sue to the side effects of medications and exposure to toxins. Such substances are grouped into 11 classes e.g.
1. Alcohol.
2. Amphetamines also similar drugs.
3. Caffeine.
4. Cannabis.
5 Cocaine.
6. Hallucinogens
7. Inhalants.
8. Nicotine.
9. Opioids.
10. PCP and similar drugs, sedatives.
11. Hypnotics or anxiolytics.
This section also deals with poly-substance dependence and other or unknown substance-related Disorders (this entails most disorders related to medications or toxins).
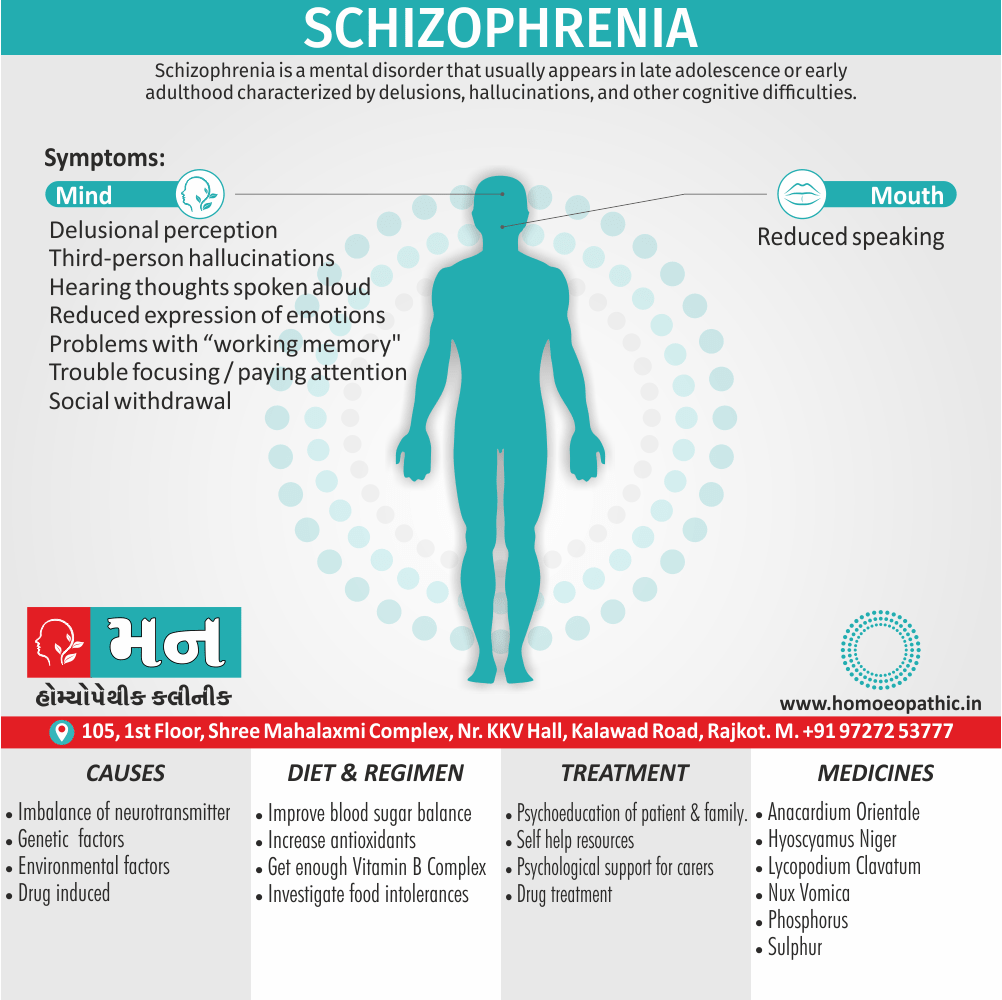
5. Schizophrenia and other psychotic disorders i.e.:
All the disorders included in this section are characterized by the presence of psychotic symptoms such as delusions and hallucinations. A broader definition would also include other symptoms such as disorganized thought process and/or speech. The most well known example from this category would be:
1. Schizophrenia.
2. Others include: schizoaffective disorder.
3. Delusional disorder.
4. Brief psychotic disorder.
5. Psychotic . disorder ( not otherwise specified).
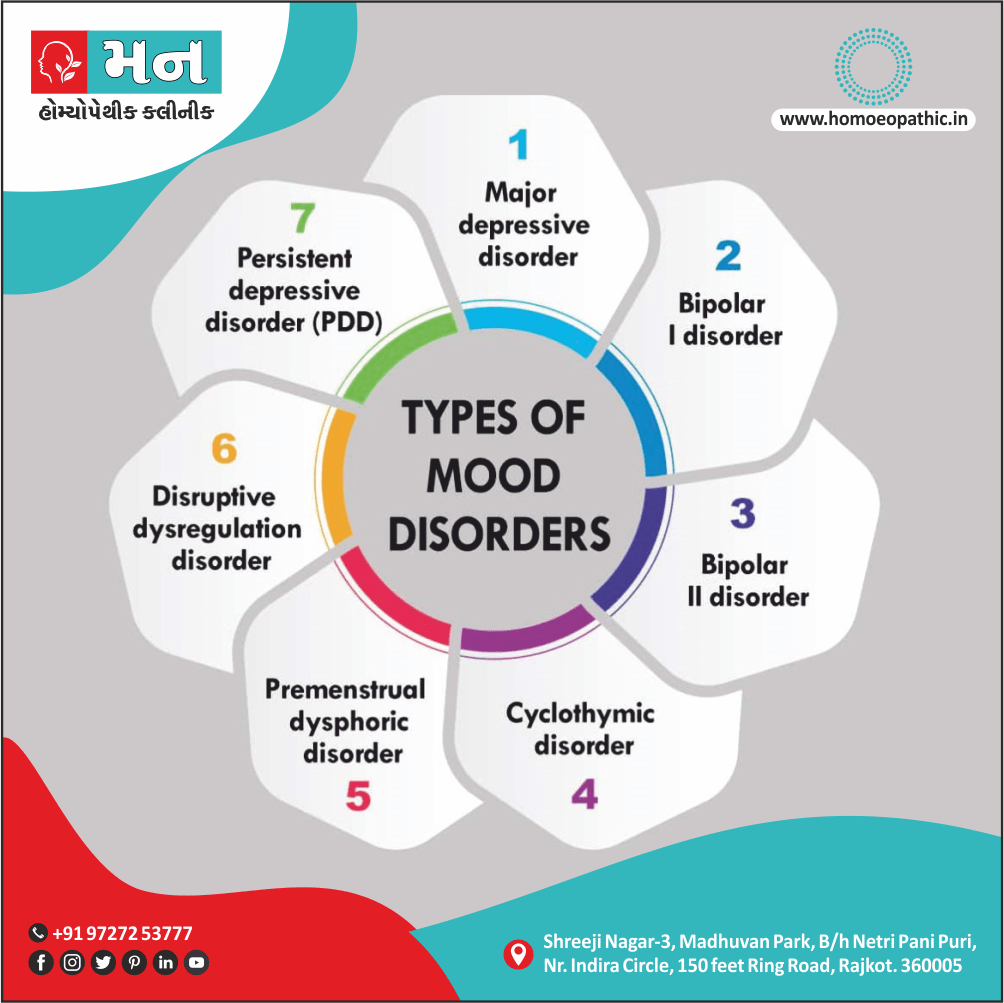
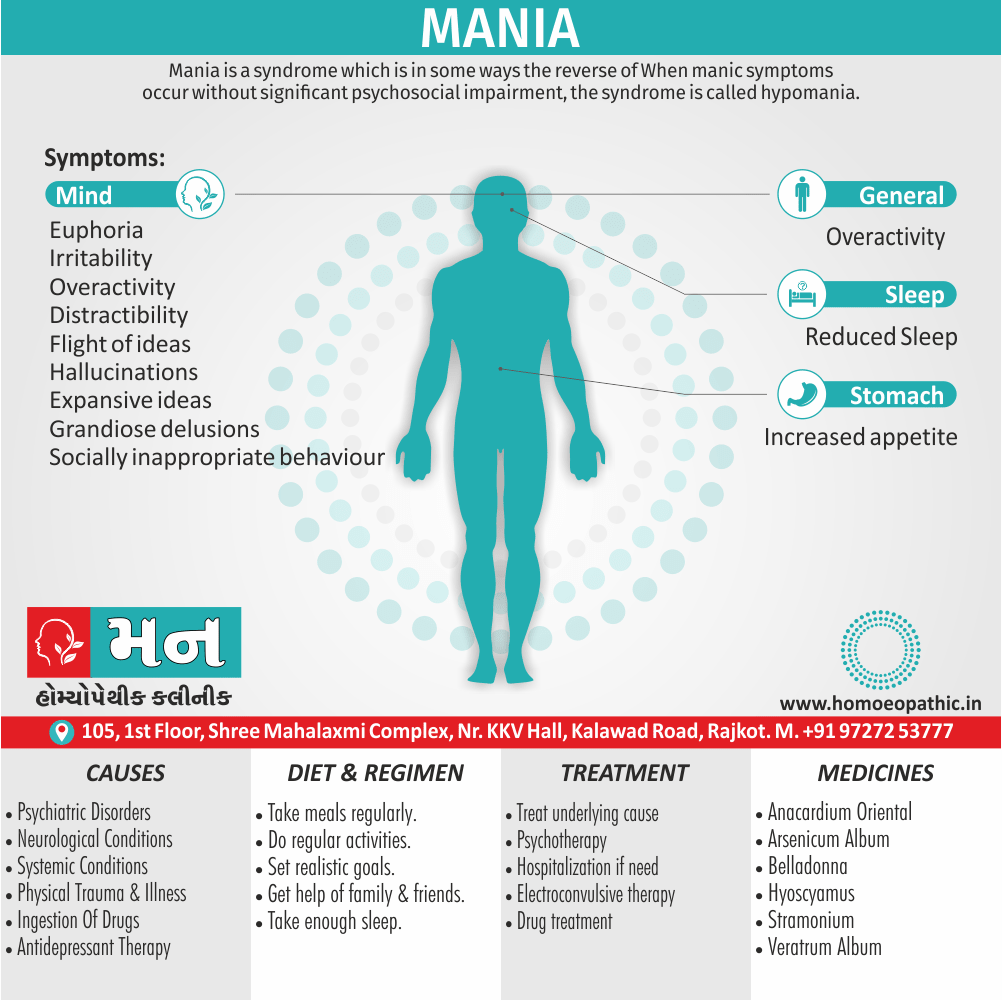
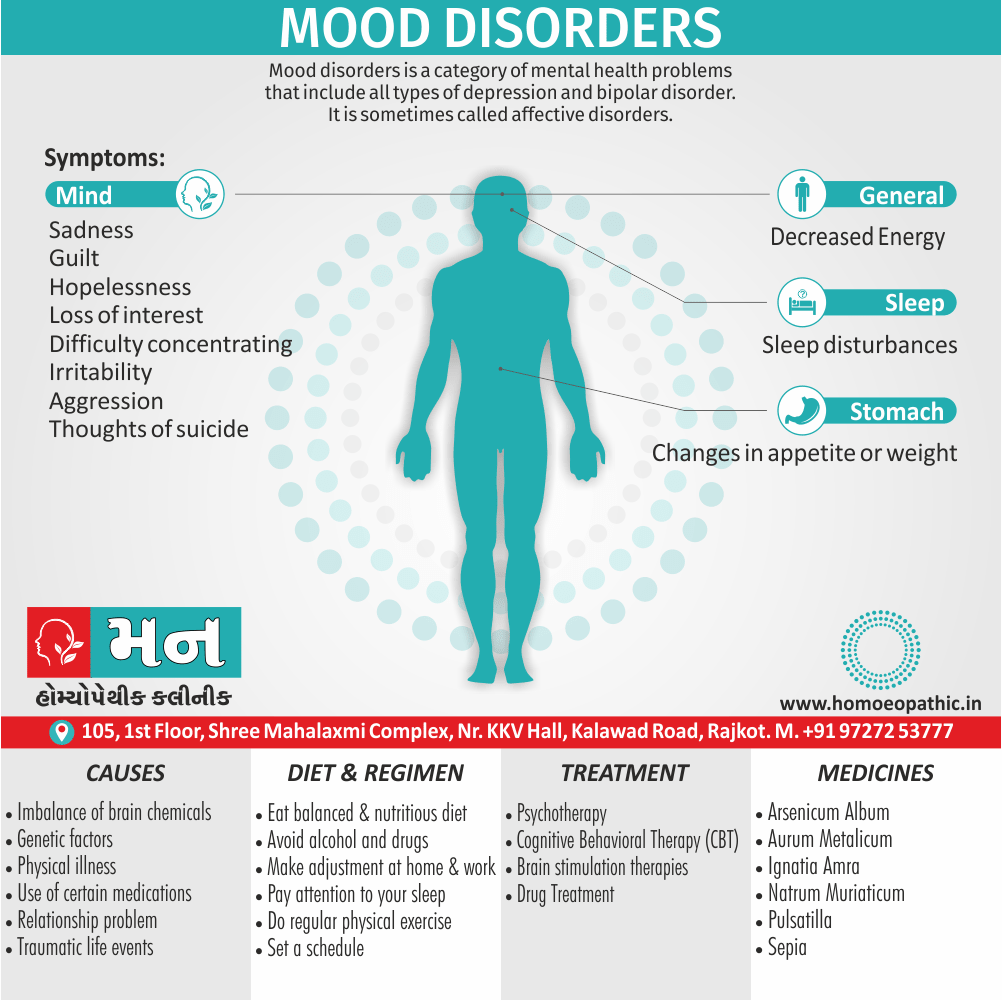
6. Mood disorders i.e.:
Disturbance in mood is the defining feature of various .disorders in this category. The disorders. are divided into:
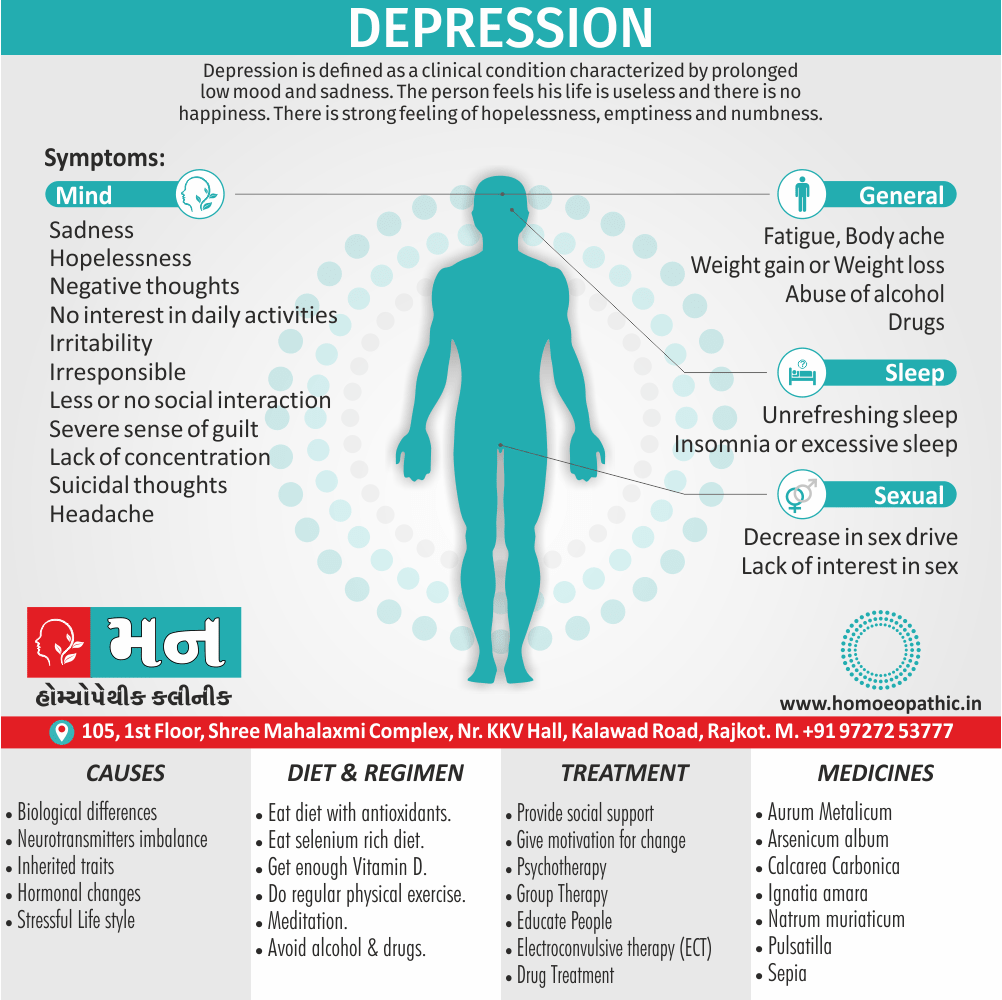
1. Depressive disorders (major depressive disorder) or “clinical depression”.
2. Dysthymic disorder.
3. Depressive disorder (not otherwise specified).
4. These are distinguished from the bipolar disorders by the fact that there is no history of a manic, hypomanic or mixed episode.
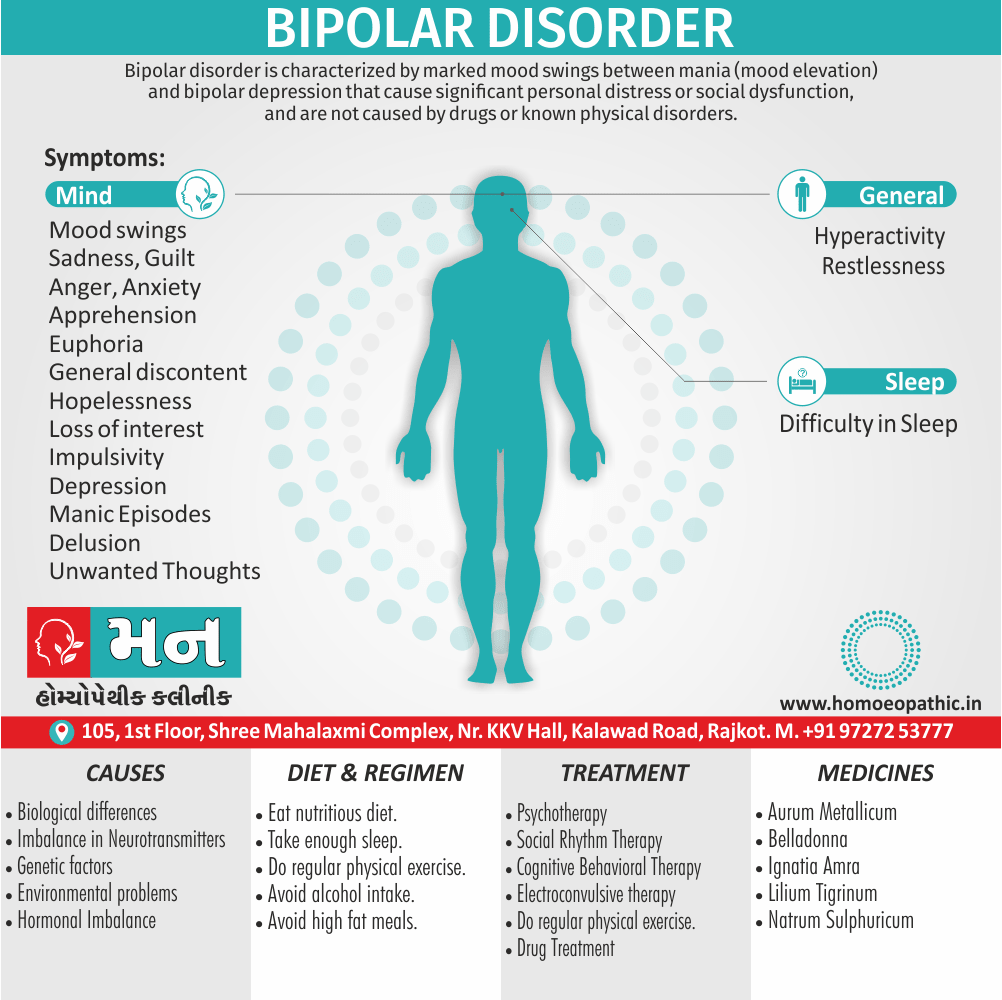
5. Bipolar disorders (Bipolar I disorder, Bipolar II disorder, Cyclothymic disorder and Bipolar disorder not otherwise specified); these disorders involve the presence ( or history) of manic, hypomanic or mixed episodes.
6. Mood disorder due to a general medical condition, substance-induced.
7. Mood disorder not otherwise specified.
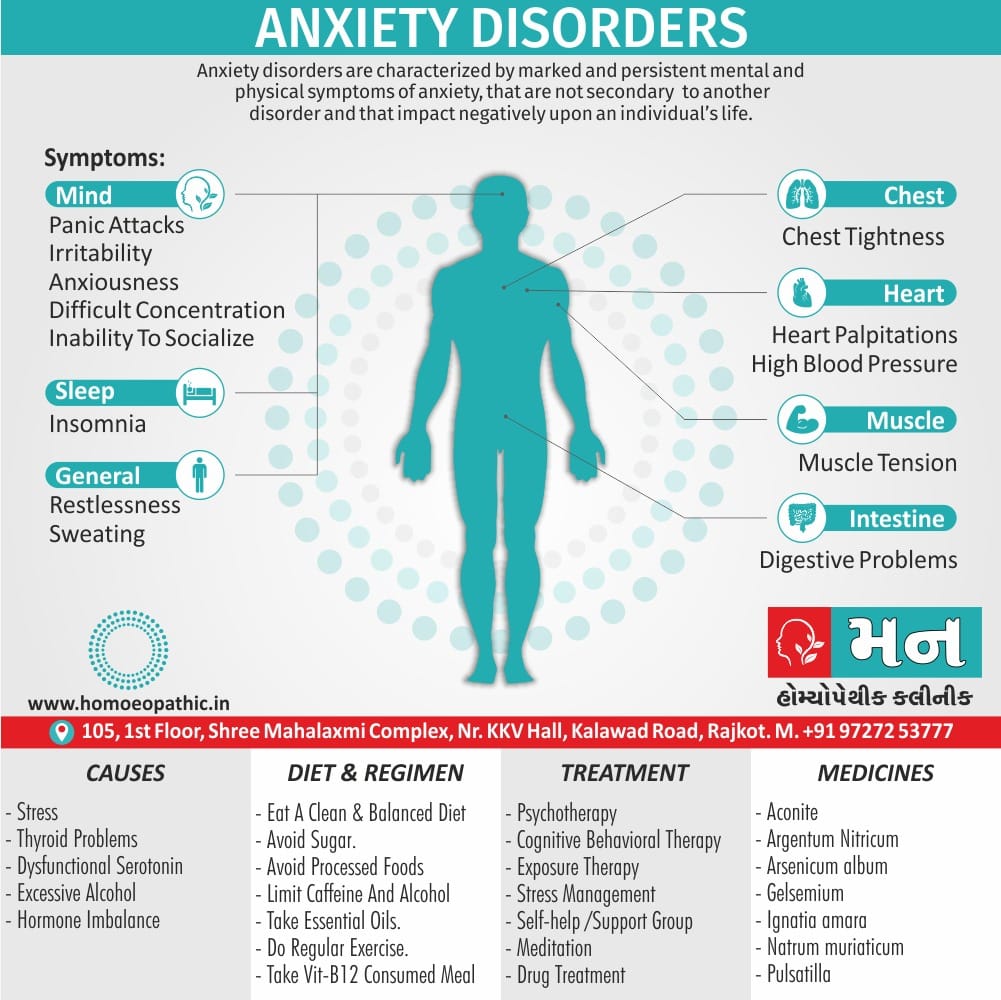
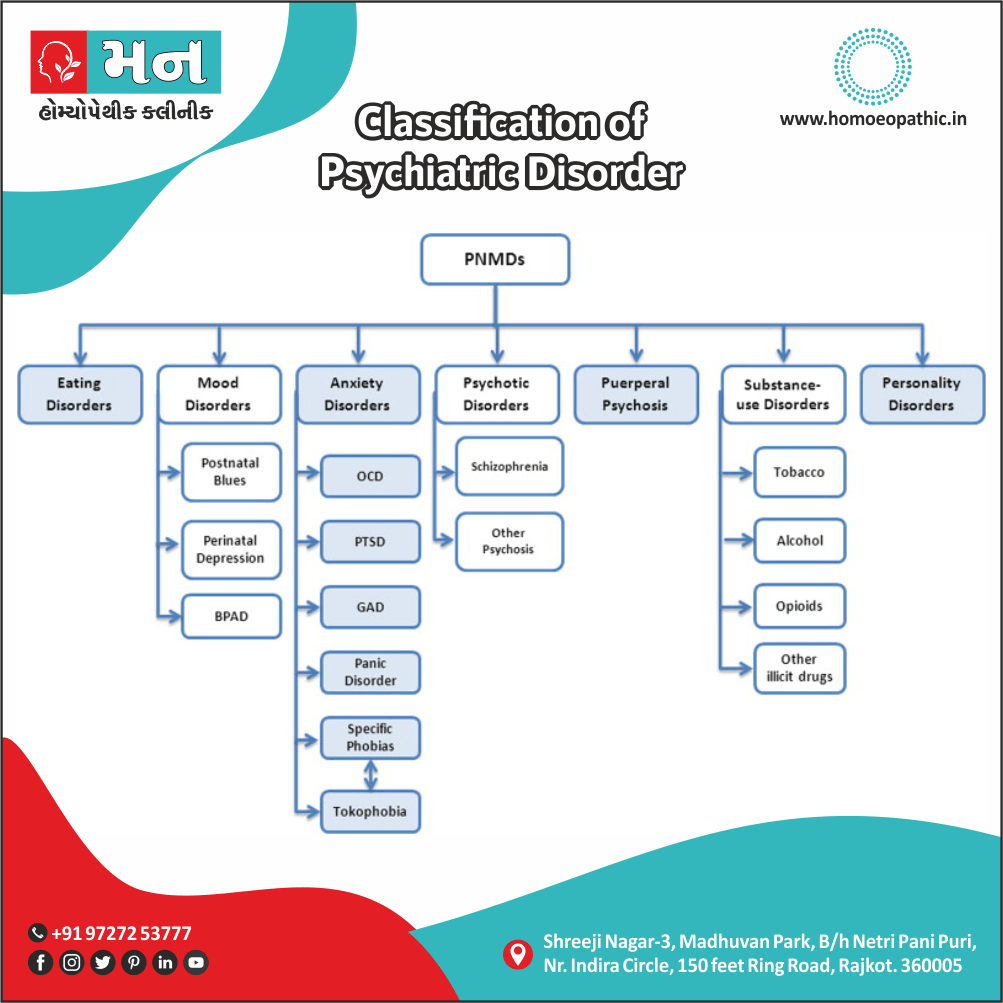
7. Anxiety disorders i.e.:
The disorders contained in this category include:
1. Panic disorder (both with and without Agoraphobia).
2. Agoraphobia (without history of Panic Disorder).
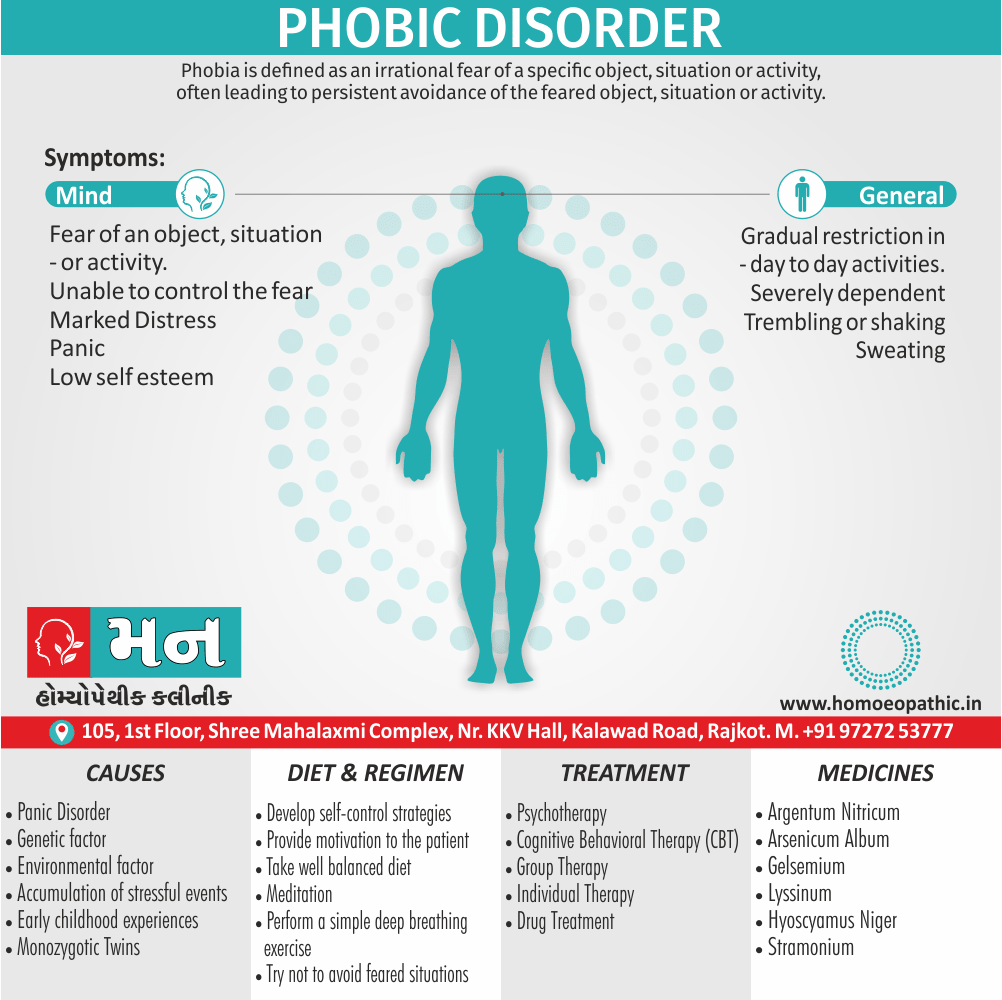
3. Specific phobias.
4. Social phobia.
5. Obsessive-compulsive disorder (in other words, OCD).
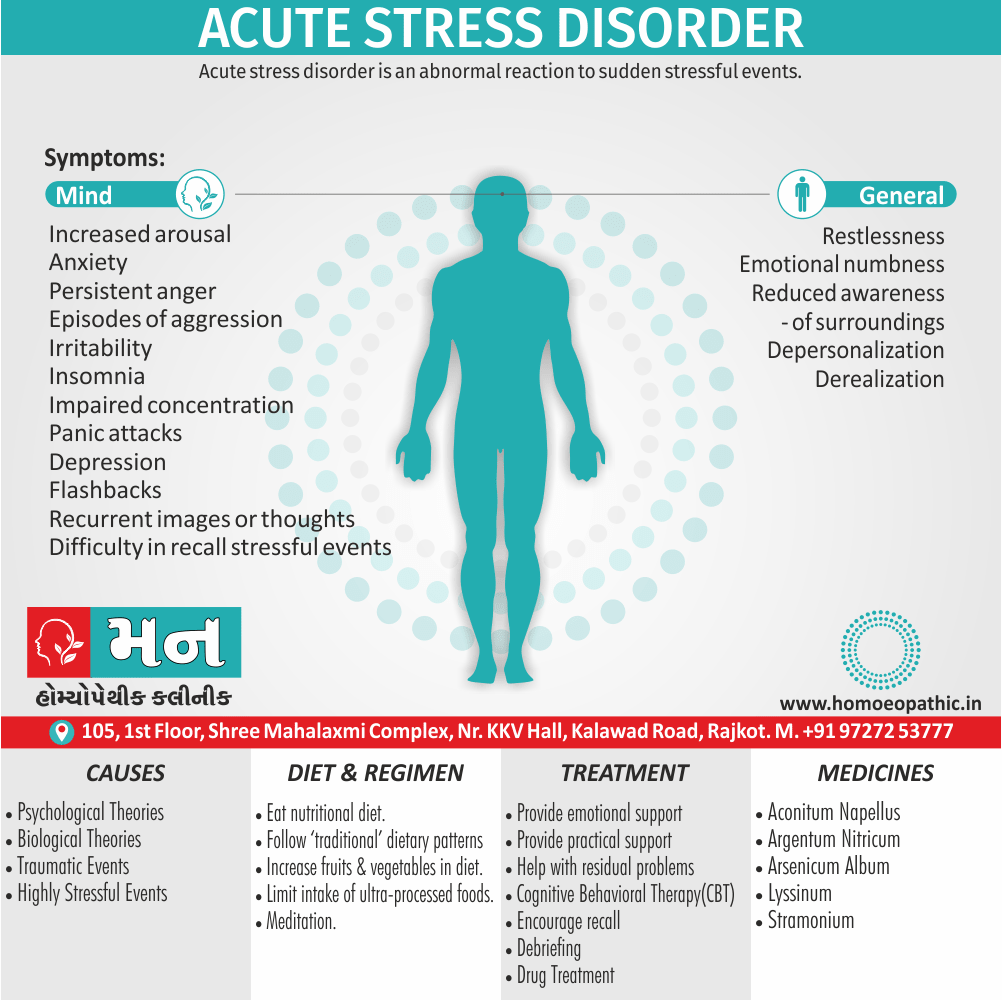
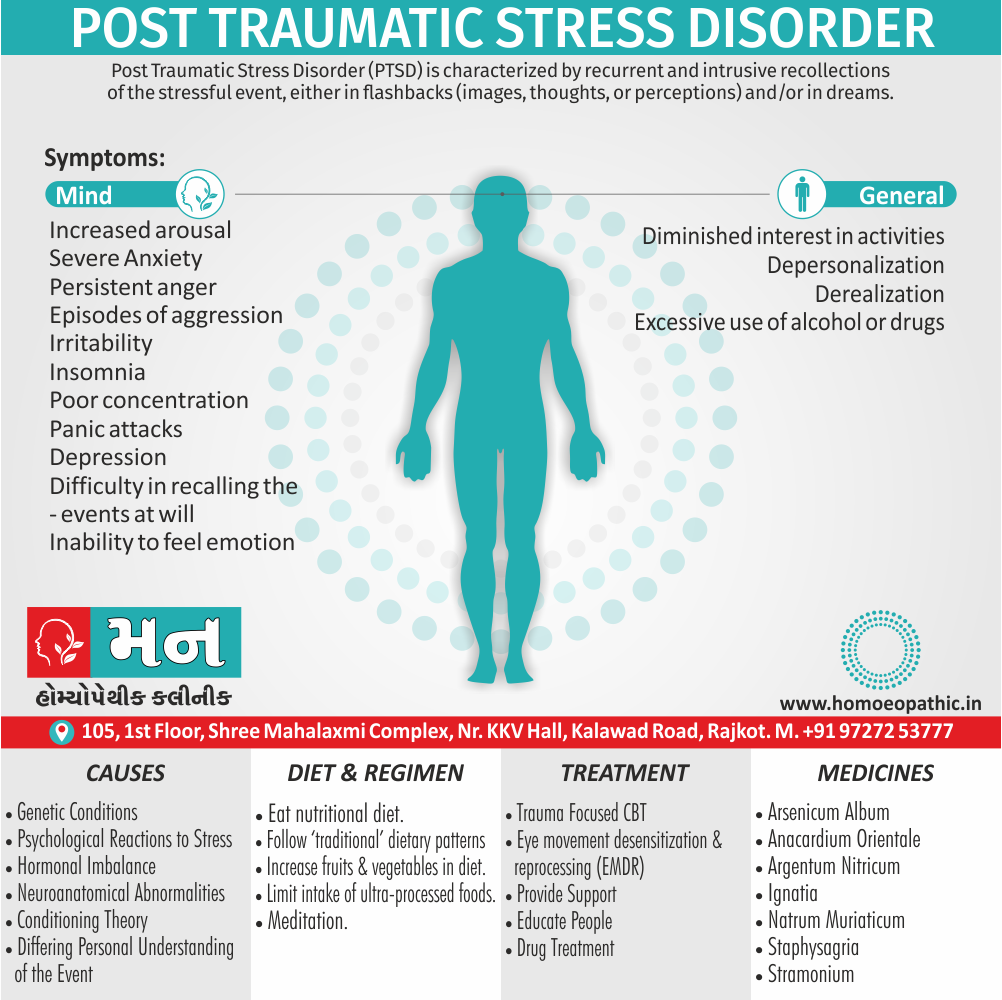
6. Post-traumatic stress disorder (in other words, PTSD), Acute stress disorder.
7. Generalized anxiety disorder, anxiety disorder due to a general medical condition.
8. Substance-Induced anxiety disorder and anxiety disorder (not other- wise specified). As the name suggests, the predominant feature of all of these disorders is the presence of anxiety-related symptoms, both physical and psychological.
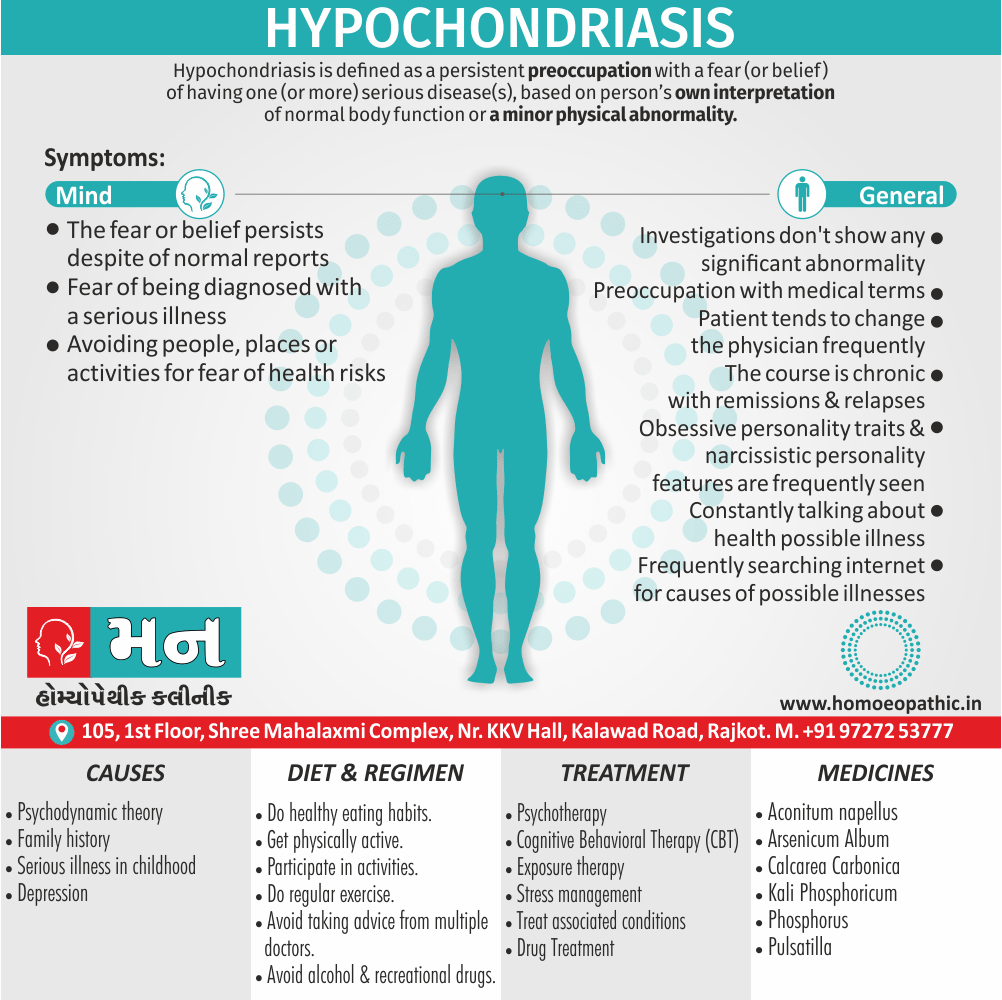
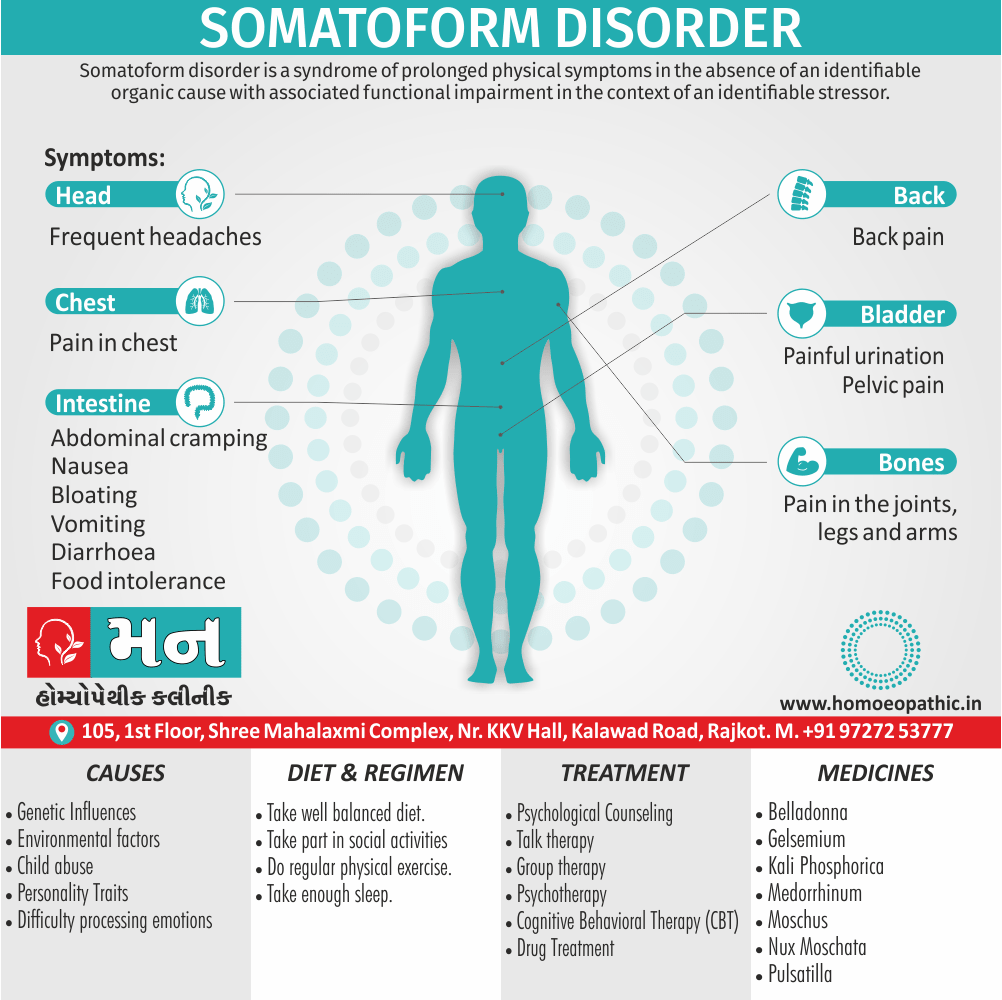
8. Somatoform disorders i.e.:
According to the DSM IV, the common feature of Somatoform disorders is the presence of physical symptoms suggesting the presence of a general medical condition but the symptoms are not fully explained either by the general medical condition or by the effects of a substance, or by another mental disorder. The production of such physical symptoms (unlike those in Factitious disorder and malingering) is not intentional, and there is no diagnosable medical condition to fully account for these physical symptoms. This category includes:
1. Somatization disorder.
2. Undifferentiated somatoform disorder.
3. Conversion disorder.
4. Pain disorder.
5. Hypochondriasis.
6. Body dysmorphic disorder.
7. Somatoform disorder (not otherwise specified).
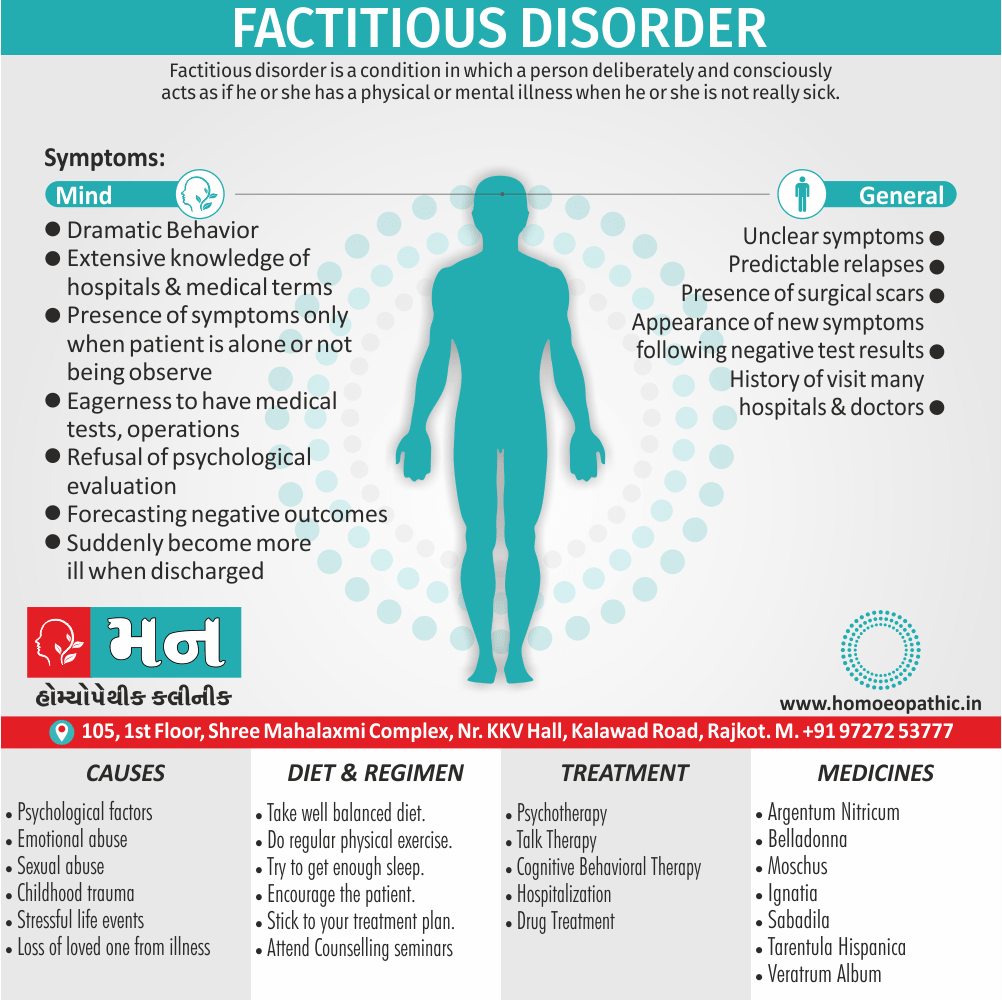
9. Factitious disorders i.e.:
1. These disorders are characterized by intentionally produced or feigned physical or psychological symptoms in order to assume the sick role.
2. In malingering, the symptoms are also feigned or produced intentionally but in this instance there is a tangible motive for doing so and such goal is obvious when the person’s circumstances are known.
3. On the other hand, in factitious disorder the motivation is purely psychological to assume the role of being sick.
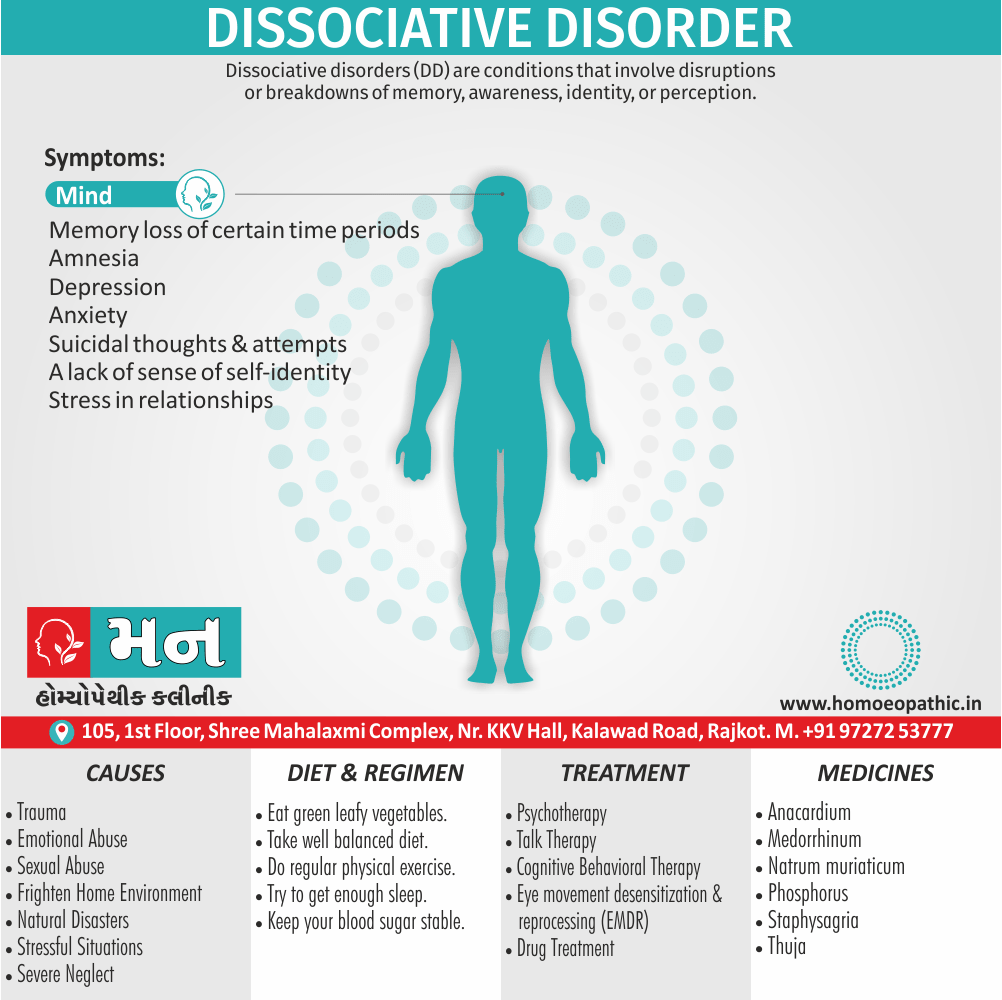
10. Dissociative disorders i.e.:
The DSM TV notes that the essential feature of dissociative disorders is a “disruption in the usually integrated functions of consciousness, memory, identity or perception of the environment”. Various disorders in this category are:
1. Dissociative amnesia.
2. Dissociative fugue.
3. Dissociative identity disorder (previously known as “multiple personality disorder).
4. Depersonalization disorder.
5. Dissociative disorder ( not otherwise specified).
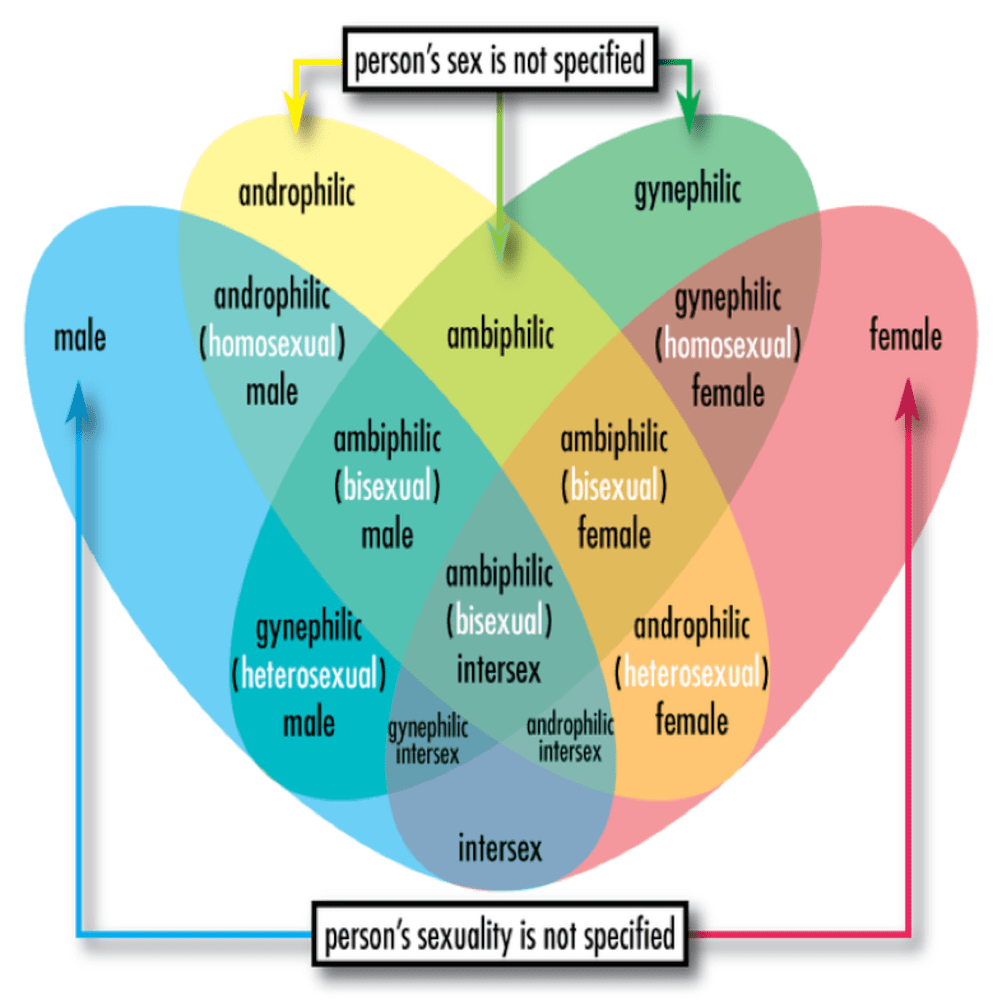
11. Sexual and gender identity disorders i.e.:
This category contains:
1. Sexual dysfunctions.
2. Paraphilias.
3.The gender identity disorders.
The former i.e.:
1.Sexual desire disorders,
2. Sexual arousal disorders.
3. Orgasmic disorders.
4. Sexual pain disorders.
5. Sexual dysfunction due to a general medical condition.
6. Substance induced sexual dysfunction.
7. Sexual dysfunction ( not otherwise specified).
The Paraphilias are characterized by “recurrent, intense sexual urges, fantasies, or behaviours that involve unusual objects, activities and situations and cause clinically significant distress or impairment in social, occupational, or other important areas of functioning”.
These i.e.:
1. Exhibitionism,
2. Fetishism,
3. Frotteurism,
4. Pedophilia,
5. Sexual masochism,
6. Sexual sadism,
7. Transvestic fetishism,
8. Voyeurism,
9. Paraphilia (not otherwise specified).
The gender identity disorders are characterized by “strong and persistent cross-gender identification accompanied by persistent discomfort with one’s assigned sex”, according to the DSM IV.
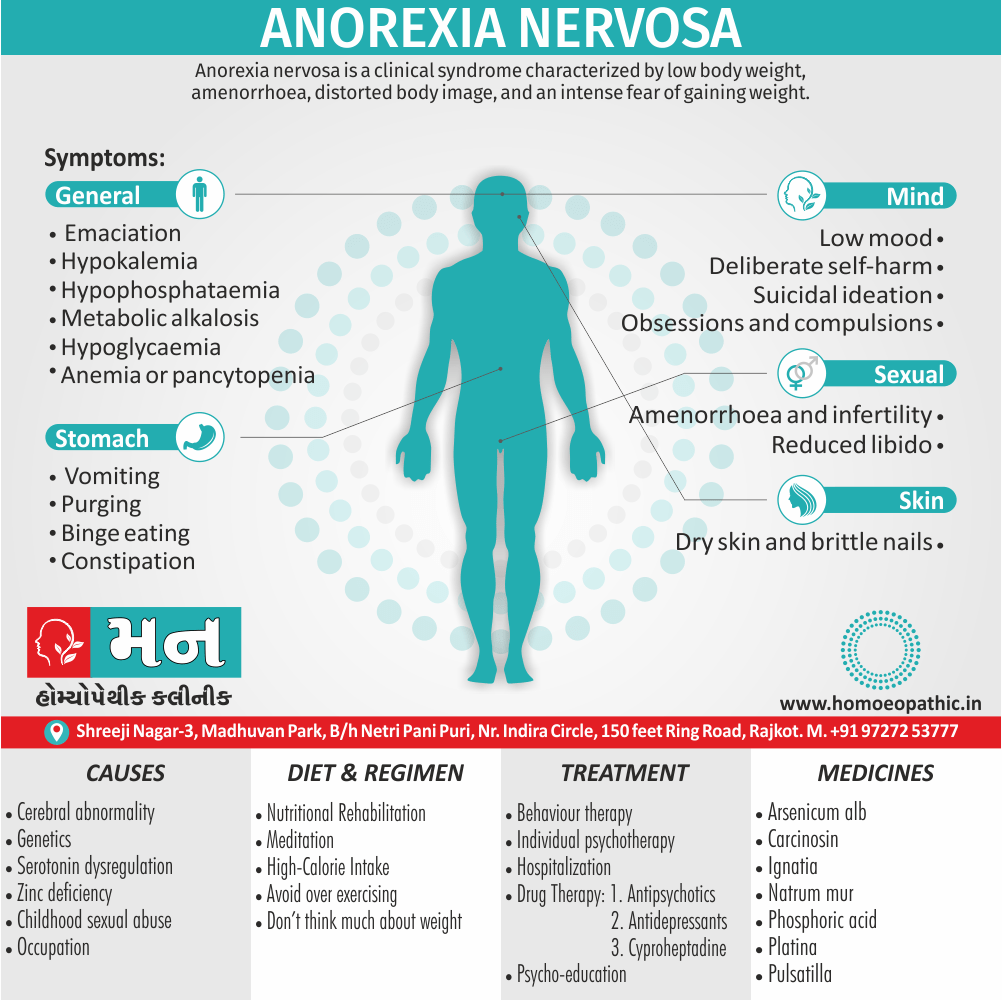
12. Eating disorders i.e.:
The predominant feature of these disorders is a severe disturbance in eating behaviour. The two specific diagnoses noted in the DSM IV are:
1. Anorexia Nervosa ( characterized by refusal to maintain a minimally normal body weight).
2. Bulimia Nervosa (characterized by repeated episodes of binge eating followed by compensatory behaviours such as self-induced vomiting, misuse of laxatives, diuretics, or other medications, fasting or excessive exercise).
An essential feature of both disorders is a distortion in perception of body shape and weight. Eating Disorder (not otherwise specified) is diagnosed when there is a clinically significant disturbance in a personal eating behaviour but the individual does not meet the criteria for a specific eating disorder.
13. Sleep disorders i.e.:
In DSM IV, sleep disorders are sub-divided according to their presumed etiology. Additionally, No specific etiology can be identified in primary sleep disorders and they consist of;
1. Dyssomnias (characterized by the abnormality in the amount, quality or timing of sleep).,
2. Parasomnias ( characterized by abnormal behaviours or physiological events occurring in association with sleep, specific sleep stages or sleep wake transitions).
In sleep disorder, related to another mental disorder there is prominent sleep disturbance resulting from another diagnosable mental disorder but of sufficient severity to warrant independent clinical attention.
The other two categories in this section are i.e.:
1. Firstly, Sleep-disorders due to a general medical condition.
2. Secondly, Substance induced sleep disorder.
14. Impulse control disorders i.e.:
The DSM IV includes the following disorders in this category:
1. Intermittent Explosive Disorder (characterized by discrete episodes of failure to resist aggressive impulses resulting in serious assaults or destruction of property).
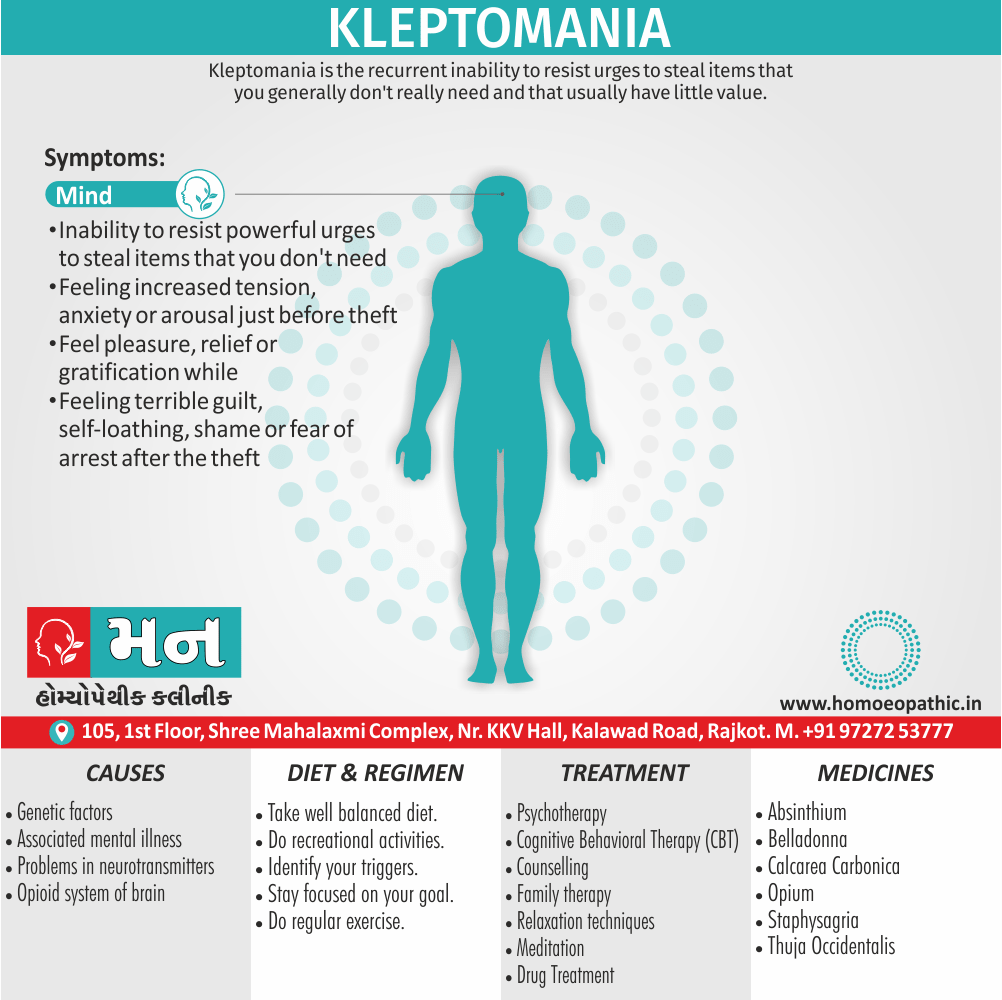
2. Kleptomania ( it characterized by recurrent failure to resist impulses to steal objects not needed either for personal use or monetary value).
3. Pyromania ( characterized by a pattern of fire setting for pleasure, either gratification or relief of tension).
4. Pathological Gambling ( characterized by either recurrent or persistent, maladaptive gambling behaviour).
5. Trichotillomania ( characterized by recurrent pulling out of one’s hair for pleasure, either gratification or relief of tension that results in noticeable hair loss).
6. Impulse Control Disorder (not otherwise specified).
15. Adjustment disorders i.e.:
The DSM IV notes the essential feature of these disorders as the onset of clinically significant emotional or behavioural symptoms in response to identifiable psychosocial stressor(s). The symptoms must develop within three months after the onset of the stressor(s).
Adjustment Disorders are sub-typed according to the predominant symptoms such as;
1. With depressed mood .
2. With anxiety.
3. With mixed anxiety also depressed mood.
4. With disturbance of conduct.
5. With mixed disturbance of emotions also conduct.
6. Unspecified.
The duration of the symptoms of Adjustment Disorders can be indicated by one of the specifiers as:
1. Acute (persistence of symptoms for less than six months).
2. Chronic (persistence of symptoms for six months or longer).
The latter requires presence of chronic stressor(s) since by definition the symptoms cannot persist for more than six months after termination of stressor(s).
16. Personality disorders i.e.:
The DSM IV defines a personality disorder as “an enduring pattern of inner experience also behaviour that deviates markedly from the expectations of the individual’s culture, is pervasive, and inflexible, has an onset in adolescence or early adulthood, is stable over time, and leads to distress or impairment”.
The manual identifies also describes diagnostic criteria for ten types specific personality disorders. These are listed below:
Paranoid Personality Disorder: characterized by a pervasive pattern of distrust also suspiciousness.
Schizoid Personality Disorder: characterized by a pervasive pattern of detachment from social relationship.
Schizotypal Personality Disorder: In brief, characterized by a pervasive pattern of acute discomfort in close relationships, cognitive also perceptual distortions and eccentricities of behaviour.
Antisocial Personality Disorder: characterized by a pervasive pattern of disregard for and violation of the rights of others.
Borderline Personality Disorder: Generally, it is characterize by a pervasive pattern of instability in interpersonal relationships, self-image, and affects and marked impulsivity.
Histrionic Personality Disorder: characterized by a pervasive pattern of excessive emotionality also attention seeking.
Narcissistic Personality Disorder: characterized by a pervasive pattern of grandiosity, need for admiration also lack of empathy.
Avoidant Personality Disorder: characterized by a pervasive pattern of social inhibition, feeling of inadequacy, also hypersensitivity to negative eval- uation.
Dependent Personality Disorder: In detail, it is characterize by a pervasive pattern of submissive and clingy behaviour related to an excessive need to be taken care of.
Obsessive Compulsive Personality Disorder: characterized by a pervasive pattern of preoccupation with orderliness, perfectionism, and control.
What Is ICD 10- Classification of Psychiatric Disorders:
1. The international classification of disease, tenth edition (ICD 10) was devised by the World Health Organization in 1993.
2. It is the most widely used system of classification in the UK.
3. The aims of ICD 10 working party were, that the scheme should:
(a) Firstly, Be suitable for international communication about statistics of morbidity and mortality.
(b) Secondly, Be a reference for national and other psychiatric classifications.
(c) Thirdly, Be acceptable and useful in research and clinical work.
(d) Lastly, Contribute to education.
Classification according to ICD 10:
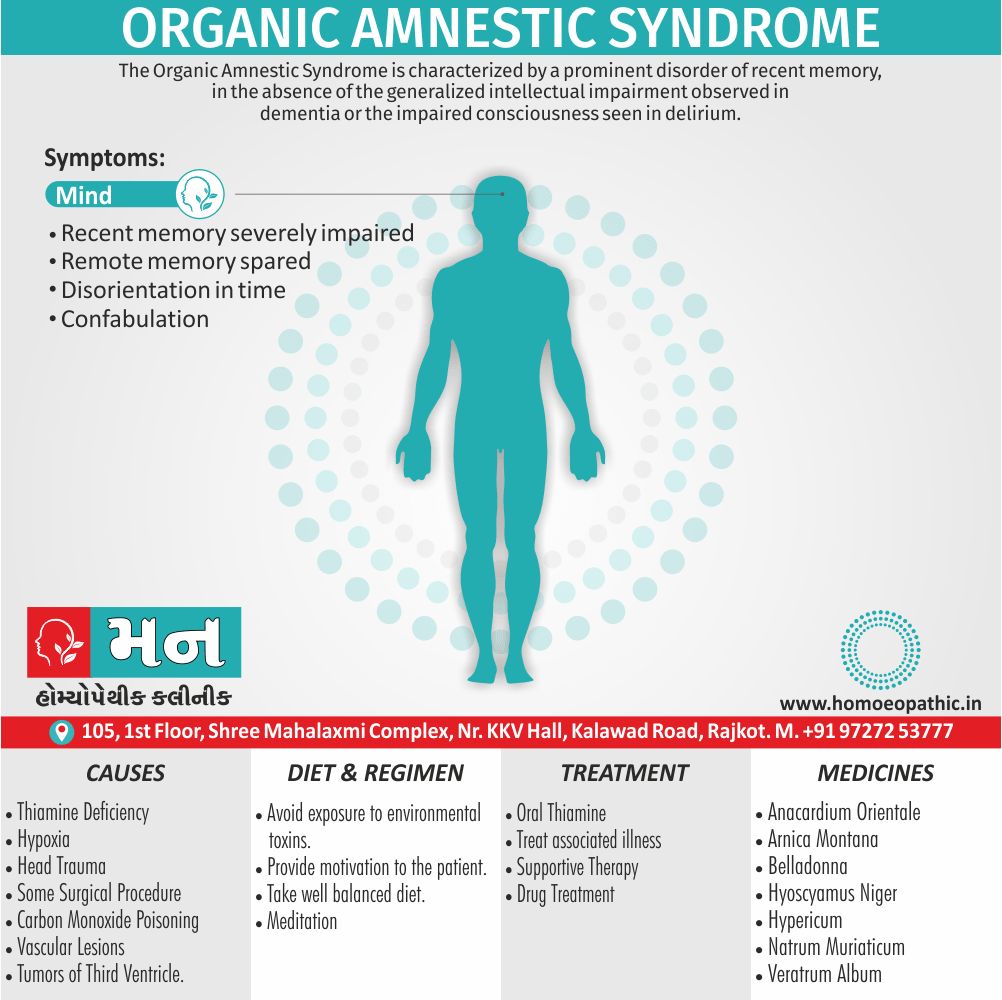
F0: Organic, including symptomatic, mental disorders.
F1: Mental and behavioural disorders due to psychoactive substance use.
F2: Schizophrenia, schizotypal, and delusional disorders.
F3: Mood (affective) disorders.
F4: Neurotic, stress related and somatoform disorders.
F5: Behavioural syndromes associated with physiological disturbances also physical factors.
F6: Disorders of adult personality also behaviour.
F7: Mental retardation.
F8: Disorders of psychological development.
F9: Behavioural and emotional disorders with onset usually occurring in either childhood or adolescence.
Classification of Psychiatric Disorders According To Homeopathy:
In Homeopathy, Hahnemann classified the mental disease in four types-
- Firstly, Somato-psychic type
- Secondly, Psychosomatic type
- Thirdly, Mental disease due to exciting cause
- Lastly, Mental disease of doubtful origin
General Classification of Psychiatric Disorders:
1. ‘Major’ disorders (Psychosis) i.e.:
(a) Organic:
i. Acute (e.g. Delirium).
ii. Chronic (e.g. Dementia).
(b) Functional:
i. Major depressive illness.
ii. Schizophrenia.
2. ‘Minor’ disorders i.e.:
(a) Psychoneurosis: anxiety, hysteria, obsession, depressive also phobic neurosis.
(b) Personality disorders: obsessional, schizoid, hysterical also sociopathic.
(c) Alcoholism also drug dependency.
(d) Psychosexual disorders.
(e) Psychosomatic disorders.
3. Mental handicap (mental retardation).
Frequently Asked Questions
Why Classification of Psychiatric Disorders is important?
In psychiatry, as in the rest of the medicine, Classification of Psychiatric Disorders is needed for three main purposes:
1. First one, To enable clinicians to communicate with one another about their patients symptoms, prognosis and treatment.
2. Second one, To ensure that research can be conducted with comparable groups of patients.
3. Lastly, To enable epidemiological studies as a basis for research and planning services.
What are the 2 system of Classification of Psychiatric Disorders?
- DSM IV
- ICD 10
Give Homeopathic Classification of Psychiatric Disorders?
- Somato-psychic type
- Psychosomatic type
- Mental disease due to exciting cause
- Mental disease of doubtful origin
What is General Classification of Psychiatric Disorders?
- ‘Major’ disorders (e.g. Psychosis)
- ‘Minor’ disorders
- Mental handicap (e.g. mental retardation)