Alcohol Use Disorder:
Definition:
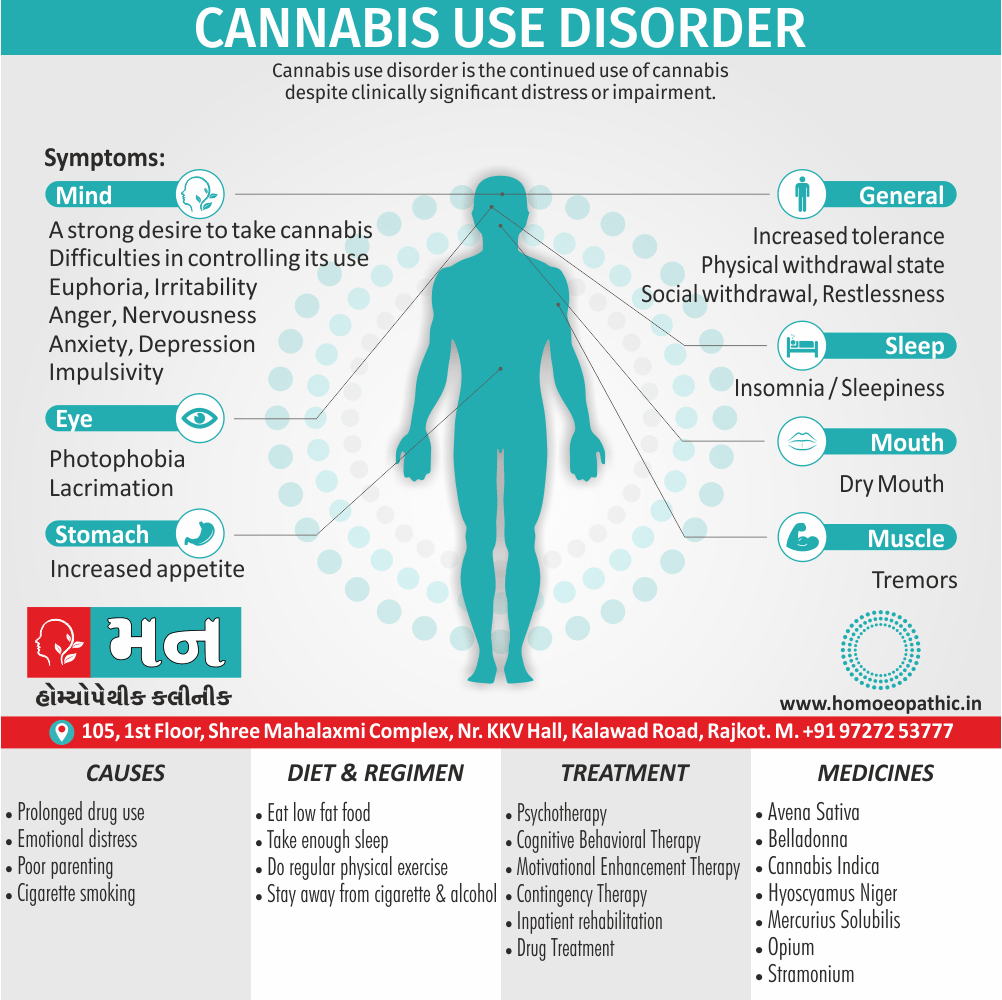
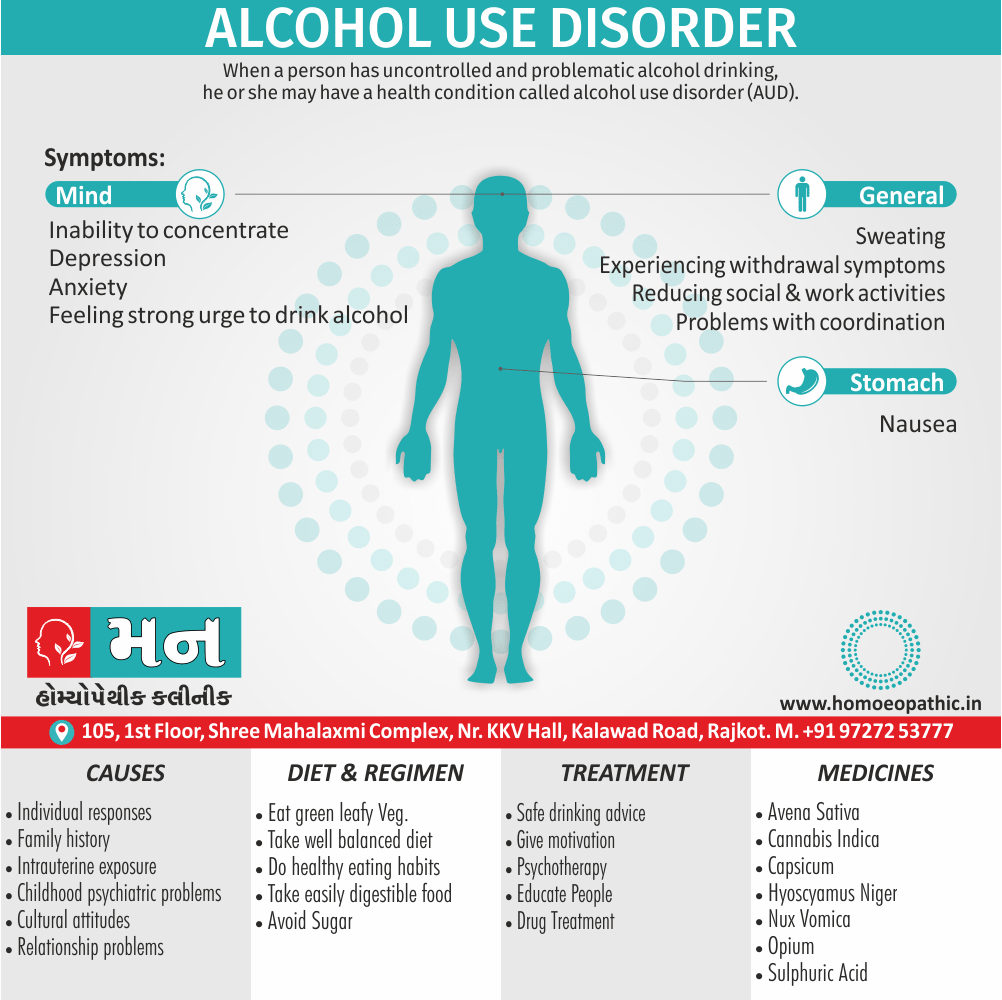
Alcohol use disorder or Alcohol dependence was previously called as alcoholism. This term much like ‘addiction’ has been dropped due to its derogatory meaning. [2]
Alcohol Use Disorder:
There are at least two billion users of alcohol worldwide, and alcohol is a major public health concern in most countries. Remembering to screen for alcohol misuse, recognizing the physical also psychological complications, and having the ability to offer basic advice and treatment are essential for all clinicians. [1]
Moving Ahead, Alcohol dependence is more common in males, and has an onset in late second or early third decade. The course is usually insidious. There is often an associated either abuse or dependence of other drugs. If the onset occurs late in life, especially after 40 years of age, an underlying mood disorder should be looked for. [2]
Causes of Alcohol Use Disorder
Biological:
- Heritable genetic factors
- Variations in alcohol metabolism
- Individual responses to alcohol
- Family history of substance abuse
- Intrauterine exposure to drugs or alcohol
Psychological:
- Risk taking and other personality traits
- Psychiatric problems in childhood (e.g. conduct disorder, abuse)
- Comorbid psychiatric disorders
Social:
- Laws affecting availability and price of alcohol
- Cultural attitudes and practices
- Peer pressure and/or role models Economic situation and employment
- Level of education
- Behavior within the family unit
- Divorce or relationship problems
Species of Alcohol Use Disorder:
According to Jellinek, there are five ‘species’ of alcohol dependence (alcoholism) on the basis of the patterns of use (also not on the basis of severity):
A. Alpha (α):
- Excessive but inappropriate drinking to relieve physical also emotional pain.
- No loss of control.
- Ability to abstain present.
B. Beta (β):
- Excessive and inappropriate drinking.
- Physical complications (e.g. cirrhosis, gastritis and neuritis) because of cultural drinking patterns and poor nutrition.
- No dependence.
C. Gamma (γ); also called as malignant alcoholism:
- Progressive course.
- Physical dependence with tolerance and withdrawal symptoms.
- Psychological dependence, also inability to control drinking.
D. Delta (δ):
- Inability to abstain.
- Tolerance.
- Withdrawal symptoms.
- The amount of alcohol consumed can be controlled.
- Social disruption is minimal.
E. Epsilon (ε):
- Dipsomania (compulsive-drinking).
- Spree-drinking.
Physical Effects of Alcohol Use Disorder
Gastrointestinal:
- Malnutrition and vitamin deficiencies (A, B, D, E, and folate)
- Carcinoma of the lip, tongue, pharynx, also larynx
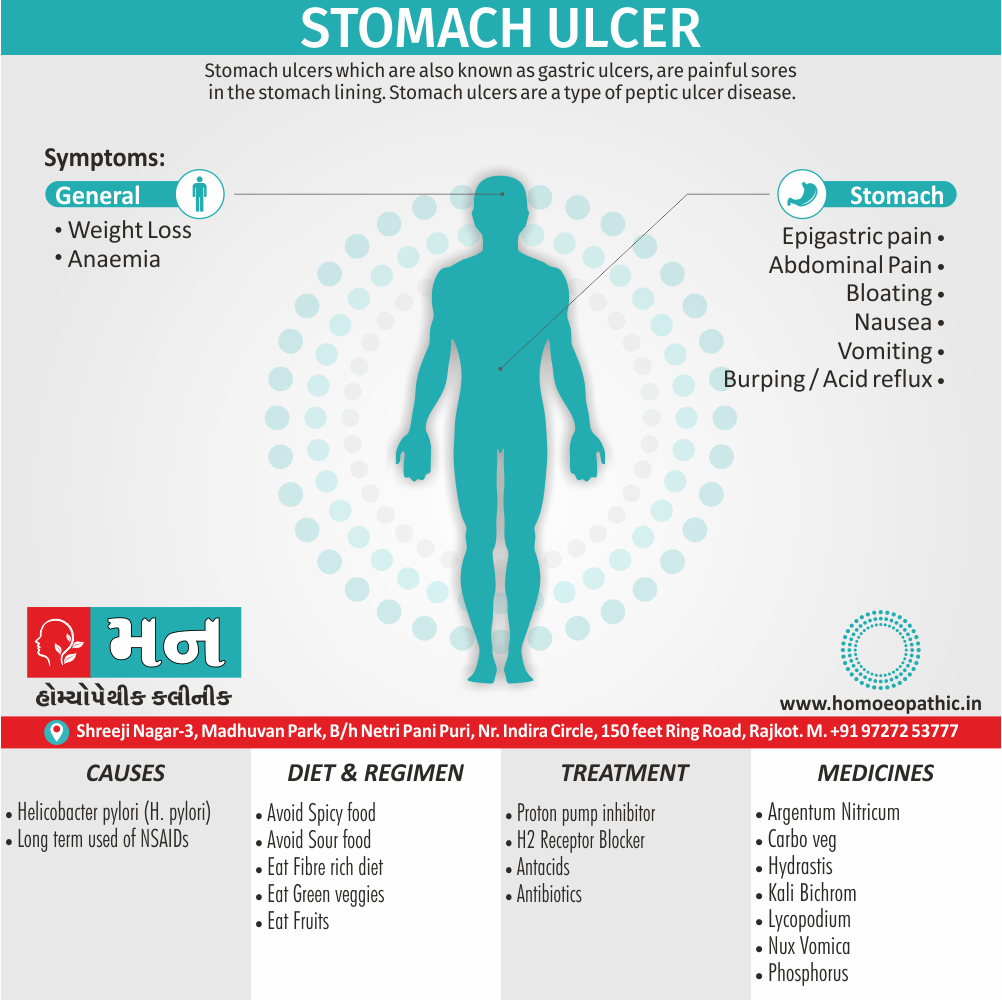
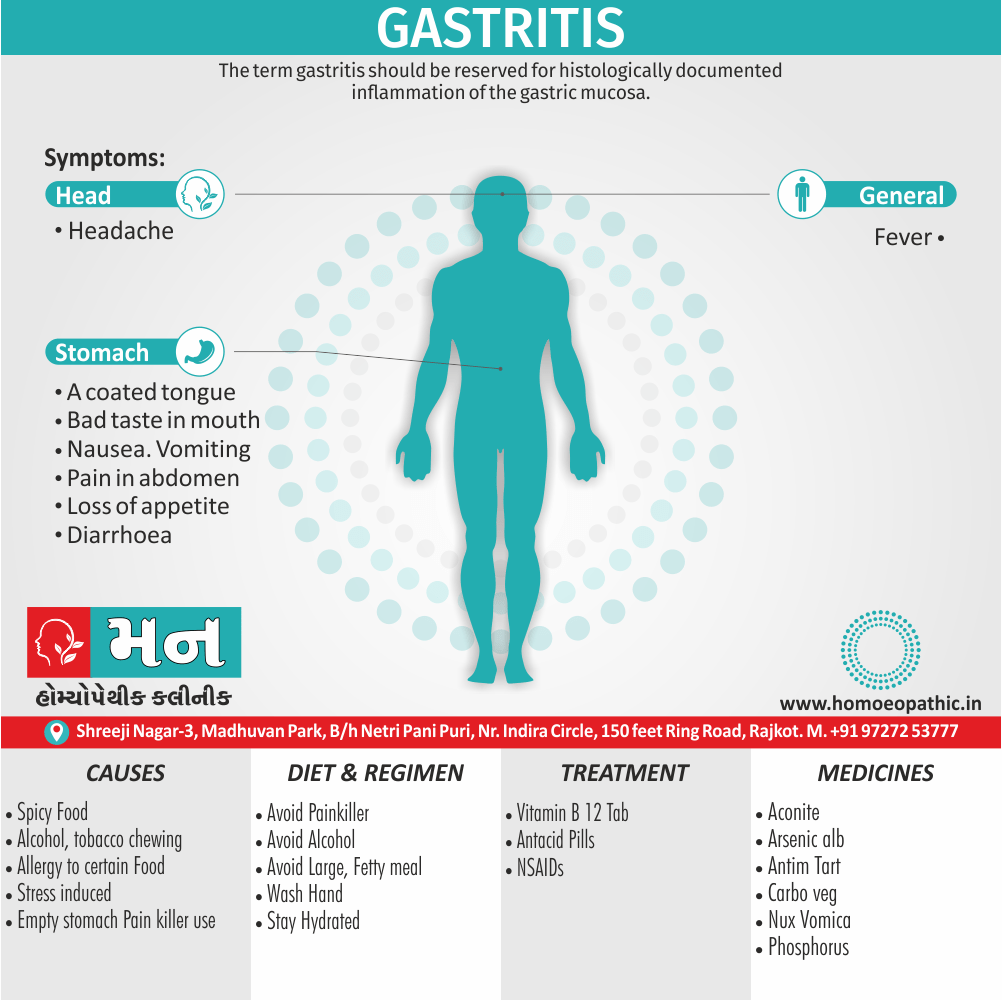
- Gastritis also peptic ulcer
- Esophageal varices
- Esophageal carcinoma
- Either Acute or chronic pancreatitis
- Fatty liver, hepatitis, cirrhosis, also primary liver carcinoma.
Neurological:
- Peripheral neuropathy
- Dementia
- Wernicke’s encephalopathy
- Korsakoff’s syndrome
- Cerebellar degeneration
- Epilepsy
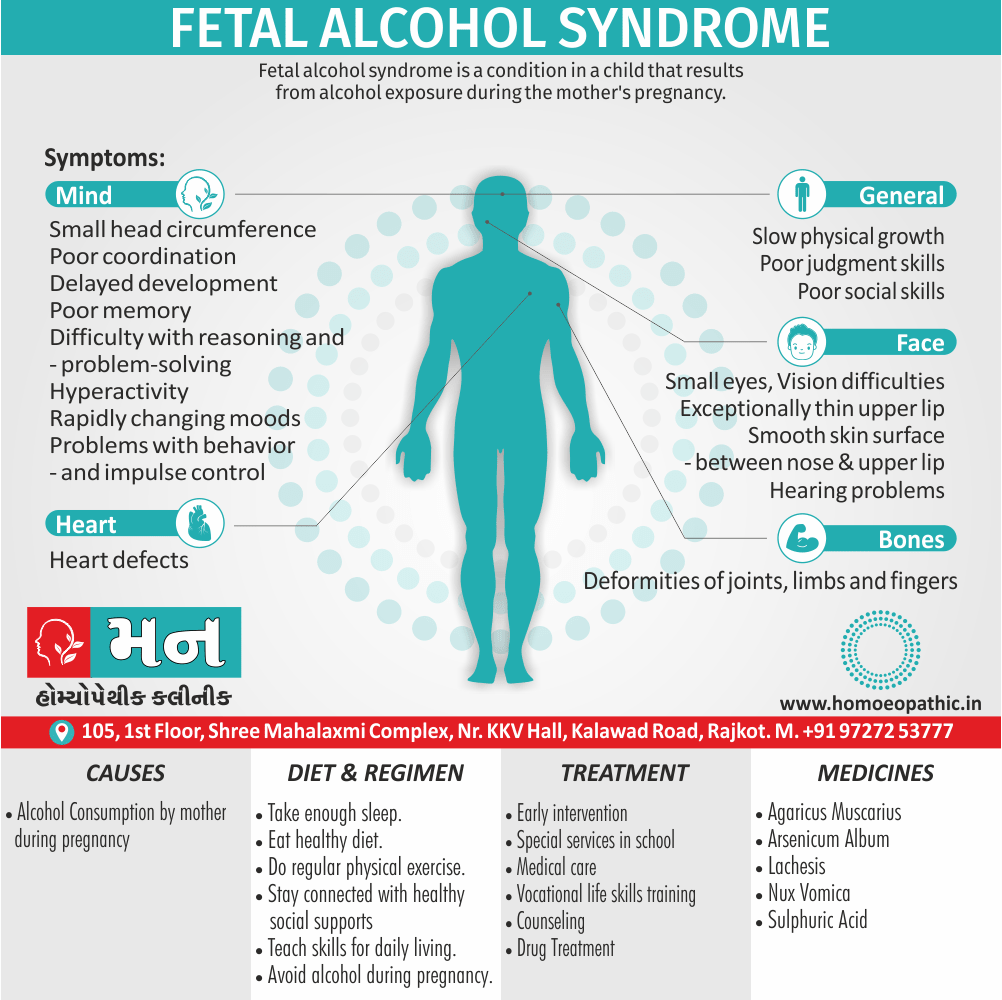
- Fetal alcohol syndrome
Other:
- Anemia, thrombocytopenia, also leukopenia
- Episodic hypoglycemia
- Haemochromatosis
- Hypertension
- Cardiomyopathy
- Myopathy
- Osteoporosis and osteomalacia
- Either Obesity or emaciation
- Facial erythema (plethora)
- Exacerbation of psoriasis
- Gout
Laboratory Markers of Alcohol Use Disorder
Certain laboratory markers of alcohol dependence have suggested.
These include:
i. GGT (γ-glutyl-transferase):
It raised to about 40 IU/L in about 80% of the alcohol dependent individuals. GGT returns to normal rapidly (i.e. within 48 hours) on abstinence from alcohol. An increase of GGT of more than 50% in an abstinent individual signifies a resumption of heavy drinking or an abnormality of liver function.
ii. MCV (mean corpuscular volume):
It is more than 92 fl (normal = 80-90 fl ) in about 60% of the alcohol dependent individuals. MCV takes several weeks to return to normal values after abstinence.
iii. Other lab markers:
It include alkaline phosphatase, AST, ALT, uric acid, blood triglycerides and CK. GGT and MCV together can usually identify three out of four problem drinkers. In addition, BAC (blood alcohol concentration) and breath analyzer can use for the purpose of identification.
For detection of the problem drinkers in the community, several screening instruments are available. MAST (Michigan Alcoholism Screening Test) frequently used for this purpose whilst CAGE questionnaire is the easiest to be administered (it takes only about 1-2 minutes).
What is a safe level of alcohol consumption?
Low levels of alcohol consumption may protect older people against coronary heart disease. Very high levels clearly do harm, but where is the dividing line between safe and unsafe consumption? A widely accepted measure is in terms of units of alcohol; one unit is 8 g of ethanol, and corresponds to the following measures in which alcohol is usually consume:
- half a pint of beer (3–4 per cent);
- a wine glass of wine (125 ml);
- either a glass of sherry or other fortified wine (50 ml);
- a standard measure of spirits (25 ml).
It is generally agreed that the ‘safe level’ of alcohol consumption is:
- Men: up to 21 units per week;
- Women: up to 14 units per week (lower because of the lower average body weight of females).
These levels assume that the whole amount is not take on one occasion and that there are occasional drink-free days. This level is equivalent, for example, to an average of three half pints of beer a day for a man.
These limits should modified in some patients; for example, pregnant women should advise to abstain from alcohol. Dangerous levels of drinking (i.e. levels of consumption at which harm is likely) are:
- Men: over 50 units per week;
- Women: over 35 units per week.
Acute intoxication of Alcohol Use Disorder
Clinical symptoms of alcohol intoxication relate jointly to the level of alcohol in the blood and the tolerance of the individual.
Increasing blood alcohol levels lead to elated or unstable mood, impaired judgement, disinhibition, impaired social and occupational functioning, cognitive impairment, ataxia, slurred speech, incoordination, nystagmus, also eventually coma.
This state leads to an increased risk of accidents (especially road traffic accidents), violence, also public order offences.
After a brief period of excitation, there is a generalized central nervous system depression with alcohol use.
With increasing intoxication, there is increased reaction time, slowed thinking, distractibility also poor motor control. There is progressive loss of self-control with frank disinhibited behavior.
Duration of intoxication
The duration of intoxication depends on the amount and the rapidity of ingestion of alcohol. Usually the signs of intoxication are obvious with blood levels of 150-200 mg%. With blood alcohol levels of 300-450 mg%, increasing drowsiness followed by coma and respiratory depression develop.
Death occurs with blood alcohol levels between 400 to 800 mg%.
Occasionally a small dose of alcohol may produce acute intoxication in some persons. This is known as pathological intoxication.
Another feature, sometimes seen in acute intoxication, is the development of amnesia or blackouts.
Firstly, The most common withdrawal syndrome is a hangover on the next morning. Mild tremors, nausea, vomiting, weakness, irritability, insomnia also anxiety are the other common withdrawal symptoms.
Lastly, Sometimes the withdrawal syndrome may be more severe, characterized by one of the following three disturbances: delirium tremens, alcoholic seizures also alcoholic hallucinosis.
1. Delirium tremens:
Delirium tremens (DT) is the most severe alcohol withdrawal syndrome. It occurs usually within 2-4 days of complete or significant abstinence from heavy alcohol drinking in about 5% of patients, as compared to acute tremulousness which occurs in about 34% of patients.
The course is short, with recovery occurring within 3-7 days. This is an acute organic brain syndrome (delirium) with characteristic features of:
- Clouding of consciousness with disorientation in time and place.
- Poor attention span and distractibility.
- Visual (and also auditory) hallucinations and illusions, which are often vivid and very frightening. Tactile hallucinations of insects crawling over the body may occur.
- Marked autonomic disturbance with tachycardia, fever, hypertension, sweating also pupillary dilatation.
- Psychomotor agitation and ataxia.
- Insomnia, with a reversal of sleep-wake pattern.
- Dehydration with electrolyte imbalance.
- Death can occur in 5-10% of patients with delirium tremens and is often due to cardiovascular collapse, infection, hyperthermia or self-inflicted injury.
2. Alcoholic seizures (‘rum fits’):
Generalized tonic clonic seizures occur in about 10% of alcohol dependence patients, usually 12-48 hours after a heavy bout of drinking. Often these patients have been drinking alcohol in large amounts on a regular basis for many years.
Multiple seizures (2-6 at one time) are more common than single seizures. Sometimes, status epilepticus may be precipitated. In about 30% of the cases, delirium tremens follows.
3. Alcoholic hallucinosis:
Alcoholic hallucinosis is characterized by the presence of hallucinations (usually auditory) during partial or complete abstinence, following regular alcohol intake. It occurs in about 2% of patients.
These hallucinations persist after the withdrawal syndrome is over, also classically occur in clear consciousness. Usually recovery occurs within one month and the duration is very rarely more than six months.
Dehydration and electrolyte disturbance are characteristic. Blood testing shows leukocytosis, raised erythrocyte sedimentation rate (ESR), and impaired liver function.
Complications of Chronic Alcohol Use:
Alcohol dependence is often associated with several complications; both medical and social.
Wernicke’s encephalopathy:
This is an acute reaction to a severe deficiency of thiamine, the commonest cause being chronic alcohol use. Characteristically, the onset occurs after a period of persistent vomiting.
The important clinical signs are:
- Ocular signs: Coarse nystagmus and ophthalmoplegia, with bilateral external rectus paralysis occurring early. In addition, pupillary irregularities, retinal hemorrhages and papilledema can occur, causing an impairment of vision.
- Higher mental function disturbance: Disorientation, confusion, recent memory disturbances, poor attention span also distractibility are quite common. Other early symptoms are apathy and ataxia.
Peripheral neuropathy and serious malnutrition are often co-existent. Neuropathologically, neuronal degeneration additionally hemorrhages are seen in thalamus, hypothalamus, mammillary bodies and midbrain.
Korsakoff’s psychosis:
As Korsakoff’s psychosis often follows Wernicke’s encephalopathy; these are together referred to as Wernicke-Korsakoff syndrome. Moreover, Clinically Korsakoff’s psychosis presents as an organic amnestic syndrome, characterized by gross memory disturbances, with confabulation. Insight is often impaired.
Marchiafava-Bignami disease:
This is a rare disorder characterized by disorientation, epilepsy, ataxia, dysarthria, hallucinations, spastic limb paralysis, also deterioration of personality also intellectual functioning. There is a widespread demyelination of corpus callosum, optic tracts also cerebellar peduncles. The cause is probably an alcohol-related nutritional deficiency.
Other Complications:
These include:
i. Alcoholic dementia.
ii. Cerebellar degeneration.
iii. Peripheral neuropathy.
iv. Central pontine myelinosis.
Social Complications:
- Accidents
- Marital disharmony
- Divorce
- Occupational problems, with loss of productive person-hours
- Increased incidence of drug dependence
- Criminality
- Financial difficulties.
Assessment:
- Extent of drinking, evidence for dependence, alcohol related disabilities, also co-morbidities.
- Arrange medical treatment for physical complications.
- Arrange psychiatric treatment for mental health problems.
Psychoeducation:
- Safe drinking advice.
- Education for either patient or family.
- Self-help materials.
Motivation for change:
- Brief interventions
- Motivational interviewing (extended brief interventions)
- Self-help materials
Safe withdrawal:
- Community based: benzodiazepines and oral thiamine.
- Inpatient based: benzodiazepines also parenteral thiamine, management of complications.
Relapse prevention and treatment of underlying issues:
- Outpatient follow-up or CBT
- Residential or day-patient programmes
- 12-step programmes (e.g. Alcoholics Anonymous)
- Marital or family therapy
- Medications: disulfiram, Acamprosate, also naltrexone
- Ongoing vitamin supplementation
- Antidepressants for depression or anxiety disorders
- Assistance with employment, accommodation, also legal issues
Pharmacological treatments:
Disulfiram:
- Disulfiram(Antabuse: 100–200 mg/day) is used, usually in specialist practice, as a deterrent to impulsive drinking. Furthermore, It interferes with the metabolism of alcohol by irreversibly blocking acetaldehyde dehydrogenase. After that, when alcohol is taken acetaldehyde accumulates with consequent flushing, headache, choking sensations, rapid pulse, and anxiety. At last, These unpleasant effects discourage the patient from drinking alcohol while taking the drug.
- Treatment with disulfiram carries the occasional risks of either cardiac irregularities or, rarely, cardiovascular collapse. So that, the drug should not be started until at least 12 hours after the last ingestion of alcohol.
- Disulfiram has unpleasant side effects, for example a persistent metallic taste in the mouth, gastrointestinal symptoms, dermatitis, urinary frequency, impotence, peripheral neuropathy, and toxic confusional states (extremely rare).
- It should not be used in patients with recent heart disease, severe liver disease, or significant suicidal ideation. The main use of disulfiram is to provide the patient with time to recover confidence that they can manage life without alcohol; also 6 months is the recommended prescription time.
Acamprosate:
- Acamprosate is a drug that enhances GABA transmission in the central nervous system. Particularly, In animals, acamprosate reduces drinking in dependent animals and reduces relapse in animals offered alcohol after a period of abstinence. RCTs have shown it to reduce cravings for alcohol in patients with alcohol dependence.
- The usual dose is 666 mg three times daily, and is started 2–7 days after cessation of drinking. Patients who benefit from it should continue for 6 months to a year.
Naltrexone:
- Naltrexone is an opiate antagonist, which inhibits the action of endogenous endorphins released when alcohol is drunk. It reduces the urge to drink, reduces the pleasurable ‘high’ produced by alcohol, also reduces the loss of control it causes.
- Short-term usage seems to reduce the risk of relapse, but is less effective than disulfiram. It is started once abstinence is achieved at 50 mg once daily.
- Patients recovering from an alcohol problem should be advised to continue taking vitamin supplements for at least 3 months after cessation of drinking.
Psychotherapy:
- The patient should be educated about the risks of continuing alcohol use, also asked to resume personal responsibility for change and be given a choice of options for change.
- Motivational enhancement therapy with or without cognitive behavior therapy and lifestyle modification is often useful, if available.
Group therapy:
- Of particular importance is the voluntary self-help group known as AA ( Alcoholics Anonymous), with branches all over the world and a membership in hundreds of thousands.
- Although the approach is partly religious in nature, many patients derive benefits from the group meetings which are non-professional in nature.
Prevention of Alcohol use disorder
As described in the sections on epidemiology, the public health implications of alcohol use disorders are vast.
In most Western populations, approximately 90% of adults drink alcohol, and many occasionally get intoxicated.
There are seven main ways in which alcohol problems in society may be reduced.
Educate people,
- effectively persuading them not to misuse alcohol. Talking in schools, harnessing community groups, and television advertisements are all effective delivery methods. School-age education programmes are particularly important. Television and billboard adverts showing the harm alcohol may cause can deliver a striking message.
Deter
harmful drinking with penalties. Laws on driving whilst intoxicated have massively reduced the number of road traffic accidents due to alcohol.
Provide alternatives to drinking alcohol and engaging in drink-related activities.
Instigate harm-reduction strategies. For example, the mandatory use of seatbelts, airbags, and low speed limits has reduced driving-related morbidity and mortality.
Regulate the availability of alcohol and its price. Increasing taxation on alcohol, limiting the hours it may be sold, and having a minimum age for purchase are all effective methods.
Promote social, cultural, and religious movements to reduce alcohol consumption.
Treat individuals who have alcohol-related problems.
Nux vomica:
Nux is the great anti.-alcoholic remedy. It corresponds to the tremor, to the nervous affection, to the headache, to the bad taste. It also corresponds to delirium tremens, where every little noise frightens and the victim finds no rest any place, springs up at night and has frightful visions. The tremor marked with ugliness and irritability and gastric disturbance. It is the remedy for the acute results of a spree; the morning big head is often large enough for the Nux cap, and the "rich brown" taste corresponds beautifully.
It is a remedy to give while the patient is still under the influence of liquor or any of the stages of alcoholism. Agaricus will sometimes control the characteristic tremor when Nux fails.
Hyoscyamus:
When delirium tremens occurs this is usually one of the first remedies indicated. The delirium is constant and loquacious, rarely inflammatory enough for Belladonna or maniacal enough for Stramonium; the pulse is small and quick and compressible, the skin is cold and clammy, the patient is tremulous and picks constantly at objects in the air. Marked sexual excitement, desire to expose person and fear of poison. The vision are those of persecution, are terrifying, and the patient makes efforts to escape. Constant insomnia is an excellent indication; outburst of laughter alerting with weeping may also occur. Dr Butler says that for the production of sleep no remedy compares with Hyoscyamus in the tincture, five or ten drops in a half glass of water, and teaspoonful doses given half-hourly.
Cannabis Indica:
A very reliable remedy in acute Alcohol Use Disorder. Some violence, talkativeness and active mind; subjects crowd upon it. Additionally, delusions and hallucination relate to exaggerated subjects time, space, etc.; face flushed, pupils dilated, perspires easily. Surprise is constantly express on the countenance.
Opium:
This is a remedy indicate in "old sinners" who have the delirium tremens over and over again. There is a constant expression of fright or terror, they have visions of animals springing up everywhere, they see ghosts, the sleep is uneasy, the breathing is stertorous. It is specifically indicate in those cases simulating apoplexy. Stramonium is suitable in habitual drunkards.
The prevailing mental characteristic is terror, all hallucinations and illusions are fright and terror producing. It has visions of animals coming at him from every corner and he tries to escape.
The face of Stramonium is bright red, not dark red as in Opium. Arsenic has visions of ghosts, also great weakness; diseases from overuse of alcohol; patients must have their accustomed drinks; great tremulousness and nervous weakness.
Suicidal tendency constantly annoyed by bugs and vermin that he sees upon his person and unceasingly tries to brush them off. Additionally, Belladonna too has delirium with visions of rats, mice, etc., and so has Calcarea Carbonica. Belladonna is easily distinguish from Opium, and Calcarea comes in as a last resort after Belladonna and Stramonium have ceased to do well.
Ranunculus bulbous
given in the tincture has found to be most calming in attacks of delirium tremens. It is undoubtedly one of our best remedies in the treatment of acute Alcohol Use Disorder. Specifically, The writer has prescribed this remedy with good results.
Cimicifuga
is useful in cases that are mentally depressed and tremor is a prominent symptom. On the other hand, The delirium is mild and the hallucinations of sight relate to small objects; there is persistent sleeplessness arid physical restlessness.
Avena sativa is a valuable remedy in alcoholism where the victim is nervous and sleepless almost to the point of delirium tremens. It is also a useful remedy in the either opium or cocaine habits. Whereas, Strophanthus has also successfully used.
Sulphuric acid :
This is the remedy for chronic alcoholism. It corresponds to inebriates on their last, who are pale and shrivelled and cold, whose stomach will not tolerate the slightest amount of food. They cannot drink water unless it is well whisked. They are quick and hasty in everything, and have a great and constant craving for brandy. It comes in long after Nux vomica, perhaps after Keely and other cures have failed over and over again. Particularly, It suits the sour breath and vomiting of alcoholic dyspepsia. "Should it produce a diarrhoea Pulsatilla is the proper antidote." ( Dr Luther Peck.) .
The constant craving for brandy reminds one of Sulphur, Nux vomica and Arsenicum, all of which have craving for spirituous liquors. Tartar emetic may useful when mucous gastric derangement predominates as after beer, with tendency to pneumonia, also accompanied by cool sweat.
Capsicum:
Capsicum in ten-drop doses of the tincture will stop the morning vomiting, sinking at the pit of the stomach and intense craving for alcohol in dipsomania, and promote the appetite. Additionally, It reduces the agitation and tremor and induces calm sleep.
Delirium tremens will often speedily relieve by Capsicum. Cantharis-continual attempts to bite; sexual excitement; face pale, yellow, dysuria. Spiritus glandium Quercus. Specifically, Burnett recommended this remedy as an antidote to the affects of alcohol, also Dr A. F. Schulz, of Fort Wayne Indiana, reported to the writer that in his opinion it would frequently cause disgust for alcoholic beverages. He has had success from its use.
Although the term alcoholism is widely used in everyday speech, it has too broad a meaning to be clinically useful. It can refer to excessive consumption of alcohol, to dependence on alcohol, or to the damage caused by excessive use.
The following terms constitute more useful categories.
Hazardous:
Hazardous drinking is a level or pattern of drinking that will eventually cause harm. It applies to anyone drinking above the recommended limits, but without current alcohol-related problems.
It is not a diagnostic term in ICD-10/DSM-IV.
Harmful drinking:
Harmful drinking refers to a pattern of use that has already caused physical, mental, or social damage to the user. Additionally, It excludes those with dependence syndrome.
Damage may be acute or chronic. It is a term used in the ICD-10 but not the DSM-IV.
Alcohol abuse:
Alcohol abuse is the term used in the DSM-IV that is most similar to harmful drinking. It involves the continued drinking of alcohol despite significant employment, social, legal, or dangerous problems resulting from it.
Dependent drinking:
Dependent drinking (ICD-10) or alcohol dependency (DSM-IV). There are seven characteristics of dependence upon alcohol, three of which must have been present in the previous year to make a diagnosis:
1. Tolerance i.e.:
Tolerance, as defined by either of the following i.e.:
- need for markedly increased amounts of alcohol to achieve intoxication or the desired effect;
- a markedly diminished effect with continued use of the same amount of alcohol.
2. Withdrawal i.e.:
Withdrawal, as defined by either of the following:
- the characteristic withdrawal syndrome for alcohol;
- alcohol is take to relieve or avoid withdrawal symptoms.
3. Alcohol is often take in larger amounts or over a longer period than was intend.
4. There is a persistent desire for or there are unsuccessful efforts to cut down or control alcohol use.
5. A great deal of time is spend in activities necessary to obtain alcohol, use alcohol, or recover from its effects.
6. Important social, occupational, or recreational activities are give up or reduced because of alcohol use.
7. Alcohol use is continue despite knowledge of having a either persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by the alcohol.
Collectively, all of these categories of disorder are best described as alcohol problems.
Frequently Asked Questions
What is Alcoholism?
Alcohol use disorder or Alcohol dependence was previously called as alcoholism. This term much like ‘addiction’ has been dropped due to its derogatory meaning.
What are the withdrawal symptoms of Alcohol use disorder ?
The most common withdrawal syndrome is a hangover on the next morning. Mild tremors, nausea, vomiting, weakness, irritability, insomnia also anxiety are the other common withdrawal symptoms.
What are the causes of Alcoholism?
- Heritable genetic factors
- Variations in alcohol metabolism
- Individual responses to alcohol
- Family history of substance abuse
- Intrauterine exposure to drugs and alcohol
- Psychiatry, Fourth Edition- Oxford Medical Publications – SRG- by Geddes, Jonathan Price, Rebecca McKnight / Ch 29.
- A Short Textbook of Psychiatry by Niraj Ahuja / Ch 4.
- Homeopathy in treatment of Psychological Disorders by Shilpa Harwani / Ch 18.
Definition:
Alcohol use disorder or Alcohol dependence was previously called as alcoholism. This term much like ‘addiction’ has been dropped due to its derogatory meaning. [2]
Overview
Epidemiology
Causes
Risk Factors
Types
Pathophysiology
Clinical Features
Sign & Symptoms
Clinical Examination
Diagnosis
Differential Diagnosis
Investigations
Safe alcohol consumption
Acute intoxication
Withdrawal Syndrome
Complications
Treatment
Prevention
Homeopathic Treatment
Diet & Regimen
Terminology
References
FAQ
Also Search As
Overview
Alcohol Use Disorder:
There are at least two billion users of alcohol worldwide, and alcohol is a major public health concern in most countries. Remembering to screen for alcohol misuse, recognizing the physical also psychological complications, and having the ability to offer basic advice and treatment are essential for all clinicians. [1]
Moving Ahead, Alcohol dependence is more common in males, and has an onset in late second or early third decade. The course is usually insidious. There is often an associated either abuse or dependence of other drugs. If the onset occurs late in life, especially after 40 years of age, an underlying mood disorder should be looked for. [2]
Epidemiology
Indian epidemiology then other
Causes
Causes of Alcohol Use Disorder
Biological:
- Heritable genetic factors
- Variations in alcohol metabolism
- Individual responses to alcohol
- Family history of substance abuse
- Intrauterine exposure to drugs or alcohol
Psychological:
- Risk taking and other personality traits
- Psychiatric problems in childhood (e.g. conduct disorder, abuse)
- Comorbid psychiatric disorders
Social:
- Laws affecting availability and price of alcohol
- Cultural attitudes and practices
- Peer pressure and/or role models Economic situation and employment
- Level of education
- Behavior within the family unit
- Divorce or relationship problems
Risk Factors
Types
5 Species of Alcohol Use Disorder:
According to Jellinek, there are five ‘species’ of alcohol dependence (alcoholism) on the basis of the patterns of use (also not on the basis of severity):
A. Alpha (α):
- Excessive but inappropriate drinking to relieve physical also emotional pain.
- No loss of control.
- Ability to abstain present.
B. Beta (β):
- Excessive and inappropriate drinking.
- Physical complications (e.g. cirrhosis, gastritis and neuritis) because of cultural drinking patterns and poor nutrition.
- No dependence.
C. Gamma (γ); also called as malignant alcoholism:
- Progressive course.
- Physical dependence with tolerance and withdrawal symptoms.
- Psychological dependence, also inability to control drinking.
D. Delta (δ):
- Inability to abstain.
- Tolerance.
- Withdrawal symptoms.
- The amount of alcohol consumed can be controlled.
- Social disruption is minimal.
E. Epsilon (ε):
- Dipsomania (compulsive-drinking).
- Spree-drinking.
Pathophysiology
Clinical Features
Tab Content
Sign & Symptoms
Physical Effects of Alcohol Use Disorder
Gastrointestinal:
- Malnutrition and vitamin deficiencies (A, B, D, E, and folate)
- Carcinoma of the lip, tongue, pharynx, also larynx
- Gastritis also peptic ulcer
- Esophageal varices
- Esophageal carcinoma
- Either Acute or chronic pancreatitis
- Fatty liver, hepatitis, cirrhosis, also primary liver carcinoma.
Neurological:
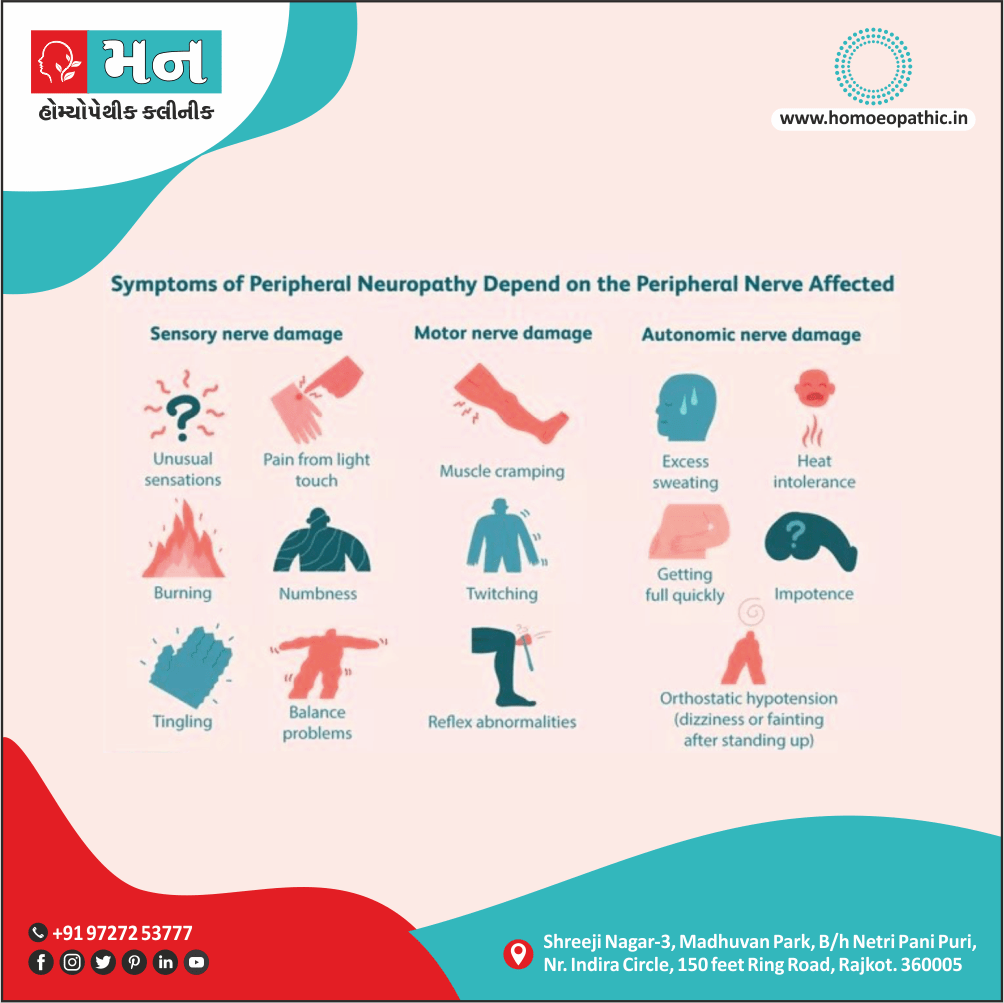
- Peripheral neuropathy
- Dementia
- Wernicke’s encephalopathy
- Korsakoff’s syndrome
- Cerebellar degeneration
- Epilepsy
- Fetal alcohol syndrome
Other:
- Anemia, thrombocytopenia, also leukopenia
- Episodic hypoglycemia
- Haemochromatosis
- Hypertension
- Cardiomyopathy
- Myopathy
- Osteoporosis and osteomalacia
- Either Obesity or emaciation
- Facial erythema (plethora)
- Exacerbation of psoriasis
- Gout
Clinical Examination
Tab Content
Diagnosis
Tab Content
Differential Diagnosis
Investigations
Laboratory Markers of Alcohol Use Disorder
Certain laboratory markers of alcohol dependence have suggested.
These include:
i. GGT (γ-glutyl-transferase):
It raised to about 40 IU/L in about 80% of the alcohol dependent individuals. GGT returns to normal rapidly (i.e. within 48 hours) on abstinence from alcohol. An increase of GGT of more than 50% in an abstinent individual signifies a resumption of heavy drinking or an abnormality of liver function.
ii. MCV (mean corpuscular volume):
It is more than 92 fl (normal = 80-90 fl ) in about 60% of the alcohol dependent individuals. MCV takes several weeks to return to normal values after abstinence.
iii. Other lab markers:
It include alkaline phosphatase, AST, ALT, uric acid, blood triglycerides and CK. GGT and MCV together can usually identify three out of four problem drinkers. In addition, BAC (blood alcohol concentration) and breath analyzer can use for the purpose of identification.
For detection of the problem drinkers in the community, several screening instruments are available. MAST (Michigan Alcoholism Screening Test) frequently used for this purpose whilst CAGE questionnaire is the easiest to be administered (it takes only about 1-2 minutes).
Safe alcohol consumption
What is a safe level of alcohol consumption?
Low levels of alcohol consumption may protect older people against coronary heart disease. Very high levels clearly do harm, but where is the dividing line between safe and unsafe consumption? A widely accepted measure is in terms of units of alcohol; one unit is 8 g of ethanol, and corresponds to the following measures in which alcohol is usually consume:
- half a pint of beer (3–4 per cent);
- a wine glass of wine (125 ml);
- either a glass of sherry or other fortified wine (50 ml);
- a standard measure of spirits (25 ml).
It is generally agreed that the ‘safe level’ of alcohol consumption is:
- Men: up to 21 units per week;
- Women: up to 14 units per week (lower because of the lower average body weight of females).
These levels assume that the whole amount is not take on one occasion and that there are occasional drink-free days. This level is equivalent, for example, to an average of three half pints of beer a day for a man.
These limits should modified in some patients; for example, pregnant women should advise to abstain from alcohol. Dangerous levels of drinking (i.e. levels of consumption at which harm is likely) are:
- Men: over 50 units per week;
- Women: over 35 units per week.
Acute intoxication
Acute intoxication of Alcohol Use Disorder
Clinical symptoms of alcohol intoxication relate jointly to the level of alcohol in the blood and the tolerance of the individual.
Increasing blood alcohol levels lead to elated or unstable mood, impaired judgement, disinhibition, impaired social and occupational functioning, cognitive impairment, ataxia, slurred speech, incoordination, nystagmus, also eventually coma.
This state leads to an increased risk of accidents (especially road traffic accidents), violence, also public order offences.
After a brief period of excitation, there is a generalized central nervous system depression with alcohol use.
With increasing intoxication, there is increased reaction time, slowed thinking, distractibility also poor motor control. There is progressive loss of self-control with frank disinhibited behavior.
Duration of intoxication
The duration of intoxication depends on the amount and the rapidity of ingestion of alcohol. Usually the signs of intoxication are obvious with blood levels of 150-200 mg%. With blood alcohol levels of 300-450 mg%, increasing drowsiness followed by coma and respiratory depression develop.
Death occurs with blood alcohol levels between 400 to 800 mg%.
Occasionally a small dose of alcohol may produce acute intoxication in some persons. This is known as pathological intoxication.
Another feature, sometimes seen in acute intoxication, is the development of amnesia or blackouts.
Withdrawal Syndrome
Firstly, The most common withdrawal syndrome is a hangover on the next morning. Mild tremors, nausea, vomiting, weakness, irritability, insomnia also anxiety are the other common withdrawal symptoms.
Lastly, Sometimes the withdrawal syndrome may be more severe, characterized by one of the following three disturbances: delirium tremens, alcoholic seizures also alcoholic hallucinosis.
1. Delirium tremens:
Delirium tremens (DT) is the most severe alcohol withdrawal syndrome. It occurs usually within 2-4 days of complete or significant abstinence from heavy alcohol drinking in about 5% of patients, as compared to acute tremulousness which occurs in about 34% of patients.
The course is short, with recovery occurring within 3-7 days. This is an acute organic brain syndrome (delirium) with characteristic features of:
- Clouding of consciousness with disorientation in time and place.
- Poor attention span and distractibility.
- Visual (and also auditory) hallucinations and illusions, which are often vivid and very frightening. Tactile hallucinations of insects crawling over the body may occur.
- Marked autonomic disturbance with tachycardia, fever, hypertension, sweating also pupillary dilatation.
- Psychomotor agitation and ataxia.
- Insomnia, with a reversal of sleep-wake pattern.
- Dehydration with electrolyte imbalance.
- Death can occur in 5-10% of patients with delirium tremens and is often due to cardiovascular collapse, infection, hyperthermia or self-inflicted injury.
2. Alcoholic seizures (‘rum fits’):
Generalized tonic clonic seizures occur in about 10% of alcohol dependence patients, usually 12-48 hours after a heavy bout of drinking. Often these patients have been drinking alcohol in large amounts on a regular basis for many years.
Multiple seizures (2-6 at one time) are more common than single seizures. Sometimes, status epilepticus may be precipitated. In about 30% of the cases, delirium tremens follows.
3. Alcoholic hallucinosis:
Alcoholic hallucinosis is characterized by the presence of hallucinations (usually auditory) during partial or complete abstinence, following regular alcohol intake. It occurs in about 2% of patients.
These hallucinations persist after the withdrawal syndrome is over, also classically occur in clear consciousness. Usually recovery occurs within one month and the duration is very rarely more than six months.
Dehydration and electrolyte disturbance are characteristic. Blood testing shows leukocytosis, raised erythrocyte sedimentation rate (ESR), and impaired liver function.
Complications
Complications of Chronic Alcohol Use:
Alcohol dependence is often associated with several complications; both medical and social.
Wernicke’s encephalopathy:
This is an acute reaction to a severe deficiency of thiamine, the commonest cause being chronic alcohol use. Characteristically, the onset occurs after a period of persistent vomiting.
The important clinical signs are:
- Ocular signs: Coarse nystagmus and ophthalmoplegia, with bilateral external rectus paralysis occurring early. In addition, pupillary irregularities, retinal hemorrhages and papilledema can occur, causing an impairment of vision.
- Higher mental function disturbance: Disorientation, confusion, recent memory disturbances, poor attention span also distractibility are quite common. Other early symptoms are apathy and ataxia.
Peripheral neuropathy and serious malnutrition are often co-existent. Neuropathologically, neuronal degeneration additionally hemorrhages are seen in thalamus, hypothalamus, mammillary bodies and midbrain.
Korsakoff’s psychosis:
As Korsakoff’s psychosis often follows Wernicke’s encephalopathy; these are together referred to as Wernicke-Korsakoff syndrome. Moreover, Clinically Korsakoff’s psychosis presents as an organic amnestic syndrome, characterized by gross memory disturbances, with confabulation. Insight is often impaired.
Marchiafava-Bignami disease:
This is a rare disorder characterized by disorientation, epilepsy, ataxia, dysarthria, hallucinations, spastic limb paralysis, also deterioration of personality also intellectual functioning. There is a widespread demyelination of corpus callosum, optic tracts also cerebellar peduncles. The cause is probably an alcohol-related nutritional deficiency.
Other Complications:
These include:
i. Alcoholic dementia.
ii. Cerebellar degeneration.
iii. Peripheral neuropathy.
iv. Central pontine myelinosis.
Social Complications:
- Accidents
- Marital disharmony
- Divorce
- Occupational problems, with loss of productive person-hours
- Increased incidence of drug dependence
- Criminality
- Financial difficulties.
Treatment
Assessment:
- Extent of drinking, evidence for dependence, alcohol related disabilities, also co-morbidities.
- Arrange medical treatment for physical complications.
- Arrange psychiatric treatment for mental health problems.
Psychoeducation:
- Safe drinking advice.
- Education for either patient or family.
- Self-help materials.
Motivation for change:
- Brief interventions
- Motivational interviewing (extended brief interventions)
- Self-help materials
Safe withdrawal:
- Community based: benzodiazepines and oral thiamine.
- Inpatient based: benzodiazepines also parenteral thiamine, management of complications.
Relapse prevention and treatment of underlying issues:
- Outpatient follow-up or CBT
- Residential or day-patient programmes
- 12-step programmes (e.g. Alcoholics Anonymous)
- Marital or family therapy
- Medications: disulfiram, Acamprosate, also naltrexone
- Ongoing vitamin supplementation
- Antidepressants for depression or anxiety disorders
- Assistance with employment, accommodation, also legal issues
Pharmacological treatments:
Disulfiram:
- Disulfiram(Antabuse: 100–200 mg/day) is used, usually in specialist practice, as a deterrent to impulsive drinking. Furthermore, It interferes with the metabolism of alcohol by irreversibly blocking acetaldehyde dehydrogenase. After that, when alcohol is taken acetaldehyde accumulates with consequent flushing, headache, choking sensations, rapid pulse, and anxiety. At last, These unpleasant effects discourage the patient from drinking alcohol while taking the drug.
- Treatment with disulfiram carries the occasional risks of either cardiac irregularities or, rarely, cardiovascular collapse. So that, the drug should not be started until at least 12 hours after the last ingestion of alcohol.
- Disulfiram has unpleasant side effects, for example a persistent metallic taste in the mouth, gastrointestinal symptoms, dermatitis, urinary frequency, impotence, peripheral neuropathy, and toxic confusional states (extremely rare).
- It should not be used in patients with recent heart disease, severe liver disease, or significant suicidal ideation. The main use of disulfiram is to provide the patient with time to recover confidence that they can manage life without alcohol; also 6 months is the recommended prescription time.
Acamprosate:
- Acamprosate is a drug that enhances GABA transmission in the central nervous system. Particularly, In animals, acamprosate reduces drinking in dependent animals and reduces relapse in animals offered alcohol after a period of abstinence. RCTs have shown it to reduce cravings for alcohol in patients with alcohol dependence.
- The usual dose is 666 mg three times daily, and is started 2–7 days after cessation of drinking. Patients who benefit from it should continue for 6 months to a year.
Naltrexone:
- Naltrexone is an opiate antagonist, which inhibits the action of endogenous endorphins released when alcohol is drunk. It reduces the urge to drink, reduces the pleasurable ‘high’ produced by alcohol, also reduces the loss of control it causes.
- Short-term usage seems to reduce the risk of relapse, but is less effective than disulfiram. It is started once abstinence is achieved at 50 mg once daily.
- Patients recovering from an alcohol problem should be advised to continue taking vitamin supplements for at least 3 months after cessation of drinking.
Psychotherapy:
- The patient should be educated about the risks of continuing alcohol use, also asked to resume personal responsibility for change and be given a choice of options for change.
- Motivational enhancement therapy with or without cognitive behavior therapy and lifestyle modification is often useful, if available.
Group therapy:
- Of particular importance is the voluntary self-help group known as AA ( Alcoholics Anonymous), with branches all over the world and a membership in hundreds of thousands.
- Although the approach is partly religious in nature, many patients derive benefits from the group meetings which are non-professional in nature.
Prevention
Prevention of Alcohol use disorder
As described in the sections on epidemiology, the public health implications of alcohol use disorders are vast.
In most Western populations, approximately 90% of adults drink alcohol, and many occasionally get intoxicated.
There are seven main ways in which alcohol problems in society may be reduced.
Educate people,
- effectively persuading them not to misuse alcohol. Talking in schools, harnessing community groups, and television advertisements are all effective delivery methods. School-age education programmes are particularly important. Television and billboard adverts showing the harm alcohol may cause can deliver a striking message.
Deter
harmful drinking with penalties. Laws on driving whilst intoxicated have massively reduced the number of road traffic accidents due to alcohol.
Provide alternatives to drinking alcohol and engaging in drink-related activities.
Instigate harm-reduction strategies. For example, the mandatory use of seatbelts, airbags, and low speed limits has reduced driving-related morbidity and mortality.
Regulate the availability of alcohol and its price. Increasing taxation on alcohol, limiting the hours it may be sold, and having a minimum age for purchase are all effective methods.
Promote social, cultural, and religious movements to reduce alcohol consumption.
Treat individuals who have alcohol-related problems.
Homeopathic Treatment
Nux vomica:
Nux is the great anti.-alcoholic remedy. It corresponds to the tremor, to the nervous affection, to the headache, to the bad taste. It also corresponds to delirium tremens, where every little noise frightens and the victim finds no rest any place, springs up at night and has frightful visions. The tremor marked with ugliness and irritability and gastric disturbance. It is the remedy for the acute results of a spree; the morning big head is often large enough for the Nux cap, and the "rich brown" taste corresponds beautifully.
It is a remedy to give while the patient is still under the influence of liquor or any of the stages of alcoholism. Agaricus will sometimes control the characteristic tremor when Nux fails.
Hyoscyamus:
When delirium tremens occurs this is usually one of the first remedies indicated. The delirium is constant and loquacious, rarely inflammatory enough for Belladonna or maniacal enough for Stramonium; the pulse is small and quick and compressible, the skin is cold and clammy, the patient is tremulous and picks constantly at objects in the air. Marked sexual excitement, desire to expose person and fear of poison. The vision are those of persecution, are terrifying, and the patient makes efforts to escape. Constant insomnia is an excellent indication; outburst of laughter alerting with weeping may also occur. Dr Butler says that for the production of sleep no remedy compares with Hyoscyamus in the tincture, five or ten drops in a half glass of water, and teaspoonful doses given half-hourly.
Cannabis Indica:
A very reliable remedy in acute Alcohol Use Disorder. Some violence, talkativeness and active mind; subjects crowd upon it. Additionally, delusions and hallucination relate to exaggerated subjects time, space, etc.; face flushed, pupils dilated, perspires easily. Surprise is constantly express on the countenance.
Opium:
This is a remedy indicate in "old sinners" who have the delirium tremens over and over again. There is a constant expression of fright or terror, they have visions of animals springing up everywhere, they see ghosts, the sleep is uneasy, the breathing is stertorous. It is specifically indicate in those cases simulating apoplexy. Stramonium is suitable in habitual drunkards.
The prevailing mental characteristic is terror, all hallucinations and illusions are fright and terror producing. It has visions of animals coming at him from every corner and he tries to escape.
The face of Stramonium is bright red, not dark red as in Opium. Arsenic has visions of ghosts, also great weakness; diseases from overuse of alcohol; patients must have their accustomed drinks; great tremulousness and nervous weakness.
Suicidal tendency constantly annoyed by bugs and vermin that he sees upon his person and unceasingly tries to brush them off. Additionally, Belladonna too has delirium with visions of rats, mice, etc., and so has Calcarea Carbonica. Belladonna is easily distinguish from Opium, and Calcarea comes in as a last resort after Belladonna and Stramonium have ceased to do well.
Ranunculus bulbous
given in the tincture has found to be most calming in attacks of delirium tremens. It is undoubtedly one of our best remedies in the treatment of acute Alcohol Use Disorder. Specifically, The writer has prescribed this remedy with good results.
Cimicifuga
is useful in cases that are mentally depressed and tremor is a prominent symptom. On the other hand, The delirium is mild and the hallucinations of sight relate to small objects; there is persistent sleeplessness arid physical restlessness.
Avena sativa is a valuable remedy in alcoholism where the victim is nervous and sleepless almost to the point of delirium tremens. It is also a useful remedy in the either opium or cocaine habits. Whereas, Strophanthus has also successfully used.
Sulphuric acid :
This is the remedy for chronic alcoholism. It corresponds to inebriates on their last, who are pale and shrivelled and cold, whose stomach will not tolerate the slightest amount of food. They cannot drink water unless it is well whisked. They are quick and hasty in everything, and have a great and constant craving for brandy. It comes in long after Nux vomica, perhaps after Keely and other cures have failed over and over again. Particularly, It suits the sour breath and vomiting of alcoholic dyspepsia. "Should it produce a diarrhoea Pulsatilla is the proper antidote." ( Dr Luther Peck.) .
The constant craving for brandy reminds one of Sulphur, Nux vomica and Arsenicum, all of which have craving for spirituous liquors. Tartar emetic may useful when mucous gastric derangement predominates as after beer, with tendency to pneumonia, also accompanied by cool sweat.
Capsicum:
Capsicum in ten-drop doses of the tincture will stop the morning vomiting, sinking at the pit of the stomach and intense craving for alcohol in dipsomania, and promote the appetite. Additionally, It reduces the agitation and tremor and induces calm sleep.
Delirium tremens will often speedily relieve by Capsicum. Cantharis-continual attempts to bite; sexual excitement; face pale, yellow, dysuria. Spiritus glandium Quercus. Specifically, Burnett recommended this remedy as an antidote to the affects of alcohol, also Dr A. F. Schulz, of Fort Wayne Indiana, reported to the writer that in his opinion it would frequently cause disgust for alcoholic beverages. He has had success from its use.
Diet & Regimen
Terminology
Although the term alcoholism is widely used in everyday speech, it has too broad a meaning to be clinically useful. It can refer to excessive consumption of alcohol, to dependence on alcohol, or to the damage caused by excessive use.
The following terms constitute more useful categories.
Hazardous:
Hazardous drinking is a level or pattern of drinking that will eventually cause harm. It applies to anyone drinking above the recommended limits, but without current alcohol-related problems.
It is not a diagnostic term in ICD-10/DSM-IV.
Harmful drinking:
Harmful drinking refers to a pattern of use that has already caused physical, mental, or social damage to the user. Additionally, It excludes those with dependence syndrome.
Damage may be acute or chronic. It is a term used in the ICD-10 but not the DSM-IV.
Alcohol abuse:
Alcohol abuse is the term used in the DSM-IV that is most similar to harmful drinking. It involves the continued drinking of alcohol despite significant employment, social, legal, or dangerous problems resulting from it.
Dependent drinking:
Dependent drinking (ICD-10) or alcohol dependency (DSM-IV). There are seven characteristics of dependence upon alcohol, three of which must have been present in the previous year to make a diagnosis:
1. Tolerance i.e.:
Tolerance, as defined by either of the following i.e.:
- need for markedly increased amounts of alcohol to achieve intoxication or the desired effect;
- a markedly diminished effect with continued use of the same amount of alcohol.
2. Withdrawal i.e.:
Withdrawal, as defined by either of the following:
- the characteristic withdrawal syndrome for alcohol;
- alcohol is take to relieve or avoid withdrawal symptoms.
3. Alcohol is often take in larger amounts or over a longer period than was intend.
4. There is a persistent desire for or there are unsuccessful efforts to cut down or control alcohol use.
5. A great deal of time is spend in activities necessary to obtain alcohol, use alcohol, or recover from its effects.
6. Important social, occupational, or recreational activities are give up or reduced because of alcohol use.
7. Alcohol use is continue despite knowledge of having a either persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by the alcohol.
Collectively, all of these categories of disorder are best described as alcohol problems.
References
- Psychiatry, Fourth Edition- Oxford Medical Publications – SRG- by Geddes, Jonathan Price, Rebecca McKnight / Ch 29.
- A Short Textbook of Psychiatry by Niraj Ahuja / Ch 4.
- Homeopathy in treatment of Psychological Disorders by Shilpa Harwani / Ch 18.
FAQ
Frequently Asked Questions
What is Alcoholism?
Alcohol use disorder or Alcohol dependence was previously called as alcoholism. This term much like ‘addiction’ has been dropped due to its derogatory meaning.
What are the withdrawal symptoms of Alcohol use disorder ?
The most common withdrawal syndrome is a hangover on the next morning. Mild tremors, nausea, vomiting, weakness, irritability, insomnia also anxiety are the other common withdrawal symptoms.
What are the causes of Alcoholism?
- Heritable genetic factors
- Variations in alcohol metabolism
- Individual responses to alcohol
- Family history of substance abuse
- Intrauterine exposure to drugs and alcohol
Also Search As
Frequently Asked Questions (FAQ)
XYZ
XXX
XYZ
XXX
XYZ
XXX
People found Homeopathic Clinic For XXXX by searching for
XXX
People found Homeopathic Doctors for XXXX by searching for
XXX
People found Homeopathic treatment for XXXX by searching for
XXX